



Every young person has to make life-changing decisions about their sexual and reproductive health. However many of them cannot access clear, evidence-based information. IPPF's comprehensive sexuality education programmes enable young people to make informed decisions about their sexuality and health, while building life skills and promoting gender equality.
Articles about Comprehensive Sex Education
12 October 2012
Exploring new territories: dialogues on comprehensive sexuality education
Exploring new territories report captures new and critical thinking about comprehensive sexuality education (CSE) sets out different pedagogical (teaching and learning) approaches identifies new priorities for CSE recognises the challenges CSE presents asks what else we need to research and discover "Comprehensive sexuality education should respond to and celebrate the diversity that exists among young people across the world. It should equip young people with knowledge, skills, attitudes and values to determine and enjoy their sexuality. Comprehensive sexuality education should take a positive and respectful approach to sexuality and sexual relationships, and be part of broader emotional and social development providing opportunities to acquire life skills and nurture personal values." This document captures a discussion designed to generate critical thinking about CSE: moving beyond developing curricula and activities to thinking about delivery and different pedagogical (teaching and learning approaches); moving beyond providing knowledge to developing skills; moving beyond public health outcomes and towards human rights and gender equality; and how to measure success. A snapshot of the challenges identified: balancing broader rights and gender equality outcomes with specific public health outcomes ensuring appropriateness in different contexts applying evidence-based approaches to both content and method pre-empting and managing resistance to new approaches What else we need to know – new areas for research developing and testing new indicators for the effectiveness and impact of CSE examining how best to foster high quality rights-based teaching and learning skills how to develop effective and continuous communication with parents and community leaders the best strategies to link CSE with health and social service provision for young people Includes: a table of ‘challenges’ ‘opportunities’ and ‘recommendations’ key questions and issues explored during the workshop a checklist of values that underpin CSE a resource list

06 July 2012
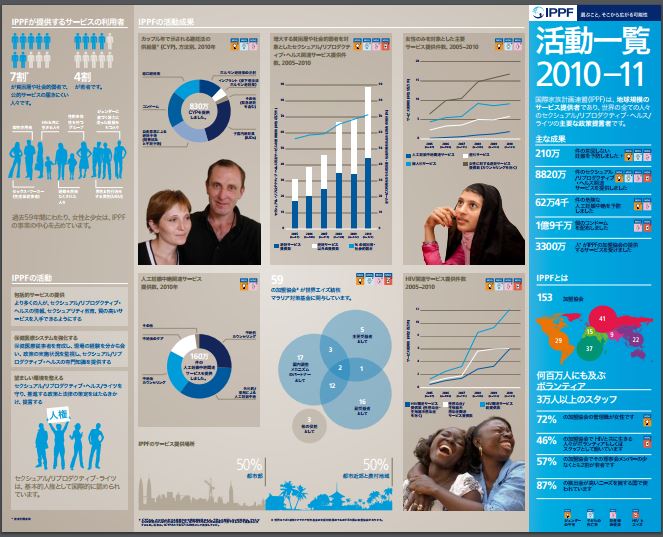
Annual Performance Report 2011-12
2012 is IPPF’s 60th year. The Annual Performance Report confirms, once again, IPPF’s vital role in human development. It opens with an overview of the external challenges that threaten sexual and reproductive health and rights (SRHR). Despite these challenges, IPPF continues to deliver impressive results. In 2011, Member Associations contributed to 116 policy and/or legislative changes in support or defence of sexual and reproductive health and rights (SRHR). The Federation as a whole provided 89.6 million SRH services with the majority going to the poor and vulnerable, including young people. Robust systems and processes have ensured that money has been invested cost-effectively where it is most needed.
12 June 2012
At a Glance 2010
Key facts and figures highlighting IPPF's achievements in 2009. Sexual and reproductive ill health causes over 30% of the global burden of disease among women of childbearing age and without IPPF, this burden would be even greater.
29 May 2012
IPPF Strategic Framework: 2005 - 2015
The product of a Federation-wide consensus, this framework brings together the ideas and experience of IPPF Member Associations, senior volunteers, Regional Offices and Central Office, and has been approved by the Governing Council. By combining an understanding of our past with a vision for our future, this new plan presents a 'framework of opportunity' that Member Associations can interpret to develop the most appropriate response to specific sexual and reproductive health challenges. The ‘Strategic Framework’ is not intended to impose a rigid set of rules or constraints. Rather, it embraces the diversity of situations Member Associations and regions face. While providing this flexibility, the framework unites the Federation in a common vision on which we are compelled to act if we are to meet the needs of women, men and young people throughout the world.

10 May 2012
Included Involved Inspired: A Framework for Youth Peer Education Programmes
The Included, involved, inspired framework promotes the benefits of youth participation through peer education guides us through planning, preparation, implementation and evaluation describes best practice provides tools to support the process of managing peer education places young people at the centre of all the processes "Peer education should support young people – both the peer educators themselves and those receiving information and services – to exercise their rights to sexual health, diversity and choice. We see peer educators as more than simply agents for behavioural change in themselves and their peers – our programmes show a commitment to also empowering them as individuals. In other words, a rights-based approach to peer education helps young people to develop the SRH knowledge, skills and attitudes needed to make their own choices regarding their sexuality and health." Peer education makes young people real stakeholders, addresses discrimination, and improves access to services. Participation means altering the power balance between young people and adults; enabling young people to identify their own problems; and ensuring that young people in all their diversity are involved in programme activities. This framework for programme designers, managers and co-ordinators, supervisors, trainers and young people can be used alongside existing guidelines and training materials to ensure peer education programmes are effective and empowering. It covers 10 stages of a peer education programme with detailed information on: Planning a peer education programme Selecting programme managers and coordinators Recruiting peer educators Training peer educators Implementing programmes: involving young people at every stage and in different roles Developing content Providing materials and condoms Supporting and keeping peer educators motivated Linking to services Monitoring, evaluation and document of programmes Includes: case studies from Nepal, the Dominican Republic, Colombia, Brazil, Sri Lanka, Peru, Guatemala, Kenya, India a check list of suggested qualities to look for, and to discuss with, a potential peer educator a check list of what makes a good training programme a case study on involving young people in monitoring and evaluation a definition of key terms a graphic of Olsson’s adapted ‘stairs of tolerance’ checklist of rules and responsibilities of a peer educator and peer counsellor 13 forms and tools for peer education programmes information on IPPF youth policies a list of peer education resources and websites

10 May 2012
From Evidence to Action: Advocating for comprehensive sexuality education
From evidence to action: advocating for comprehensive sexuality education defines CSE, answers common questions and sorts fact from fiction connects good quality CSE to global health goals promotes approaches which recognise young people’s lived experience links to reports on what works and what obstructs CSE and SRHR goals provides a checklist of activities for CSE advocates "Good sexuality education is essential to help young people to prepare for healthy and fulfilling lives. High quality information and comprehensive sexuality education can equip them with the knowledge, skills and attitudes they need to make informed choices now and in the future; to enhance their independence and self-esteem; and to help them to experience their sexuality and relationships in a positive and pleasurable way." There is evidence that CSE is effective and that abstinence-only approaches are ineffective. Evidence can provide the basis for promoting new thinking, and changing national approaches to teaching by demonstrating that a rights-based approach is a highly successful teaching methodology. It answers these questions: What is CSE? Why do it? What should it include? How can we deliver it? How can we advocate for it? This resource can help develop a greater understanding of IPPF’s vision for rights-based CSE; provide the evidence base for CSE, identifying successful characteristics, approaches and outcomes; support advocacy work with practical advice on creating the climate for CSE programmes; respond to challenges and difficult questions on comprehensive sexuality education from members of the community, addressing opposition and resistance; and create a better understanding of the links between comprehensive sexuality education and HIV prevention, human rights, health outcomes and global health goals. Young people need a realistic approach to their sexual and reproductive health: looking at psychological, socio-cultural and ethical dimensions and beyond the simply biological. CSE programmes should be rights-based; address gender and pleasure; provide choice; develop critical thinking skills; and reach vulnerable and marginalised groups. Includes: a checklist of activities to advocate for CSE ways in which comprehensive sexuality education helps further global health goals including gender equality, maternal health and combating HIV/AIDS international human rights conventions and documents that support the case for CSE links to HIV prevention a reading list of research and briefings on CSE answers to a range of common questions and myths about young people, sexual health and sexuality education answers to questions about the how, when, where and what of sexuality education A checklist of activities to advocate for comprehensive sexuality education p.16

03 May 2012
IPPF Sexual Rights Declaration Pocket Guide
02 May 2012
Sexual Rights: An IPPF declaration (abridged)
The IPPF declaration is grounded in and informed by international agreements such as United Nations Conventions. This abridged version to be used in conjunction with IPPF's original Sexual Rights Declaration.

19 April 2012
Participate: The voice of young people in programmes and policies
This is part of the Inspire pack of resources on young people's sexual and reproductive health services and programmes, for health providers and practitioners.

11 March 2019
Myths and facts about external condoms
This page was originally published in 2012 and has since been updated. External condoms (sometimes referred to as 'male' condoms) are placed over an erect penis. Learn how to put one on and find out about internal condoms. Back to external condoms – join us as we bust some common myths about this popular contraceptive method. Myth: Complications with method Some clients who seek family planning incorrectly believe that external condoms can easily get lost in a vagina or uterus and can travel through a woman’s body, requiring surgery to get the condom out. Fact: Studies indicate that a condom rarely slips off completely during intercourse. On average, about 2% of condoms break or slip off completely during sex, primarily because they are used incorrectly. Slippage during withdrawal can be minimized if the rim of the condom is held against the base of the penis during withdrawal after ejaculation. However, if a condom does slip, it will go no further than the woman’s vagina, where it can be easily retrieved, with no need for surgery. If a man notices a break or slip, he should tell his partner so that she can use emergency contraceptive pills if she wants. Myth: Effectiveness Some people who seek family planning do not want to use external condoms because they incorrectly believe that condoms are not effective in preventing pregnancy or sexually transmitted infections, including HIV. Fact: The external condom is a sheath, or covering, that fits over an erect penis. It works by forming a barrier that keeps sperm out of the vagina, preventing pregnancy. It also keeps infections that are in semen, on the penis, or in the vagina from infecting the other partner. It is usually made of very thin latex rubber, although a minority are made of either animal tissue or polyurethane (plastic). Condoms are the only contraceptive method that can protect against both pregnancy and sexually transmitted infections (STIs), including HIV transmission, when used for vaginal, oral, or anal sex. In order for condoms to be most effective they must be used correctly and consistently (with every act of sex). The risk of pregnancy or contracting sexually transmitted infections is greatest when condoms are not used correctly with every act of sex. When used correctly and consistently, condoms are 98% effective in preventing pregnancy. This means that when used consistently and correctly, about 2 of every 100 women whose partners use condoms become pregnant over the first year of use. Condoms do not have holes that HIV can pass through. In fact, when used consistently and correctly, condom use prevents 80% to 95% of HIV transmission that would have occurred without condoms. Plastic condoms are expected to provide the same protection as latex condoms, but they have not been studied thoroughly. Condoms made from animal membrane DO NOT protect against HIV and other STIs. On average, about 2% of condoms break or slip off completely during sex, primarily because they are used incorrectly. Used properly, condoms seldom break. Lubrication helps avoid condom breakage. There are three ways to provide lubrication—natural vaginal secretions, adding a lubricant, or using condoms packaged with lubricant on them. Sometimes lubricants made of glycerine or silicone, which are safe to use with latex condoms, are available. Clean water and saliva also can be used for lubrication. Do not use products made with oil as they can damage latex condoms. QUICK POLL: Are external condoms your contraceptive of choice?YesNo Myth: Health risks and side effects Some people incorrectly believe that using external condoms can cause side effects or health risks such as illness, infection, disease, or cancer. Fact: There are no known serious short or long term side effects associated with the use of condoms. When a condom is used, ejaculation occurs as normal, so there is no sperm “back up.” There is no evidence that condoms cause cancer, either in men or women. In fact, the use of condoms may help protect against conditions caused by STIs including recurring pelvic inflammatory disease, cervical cancer, and infertility. It is possible that a person may experience mild irritation in or around the vagina or penis or mild allergic reaction to a condom (itching, redness, rash, and/or swelling of genitals, groin, or thighs during or after condom use). Severe allergic reactions involve hives or rash over much of the body, dizziness, difficulty breathing, or loss of consciousness after coming in contact with latex. Both men and women can be allergic to latex and latex condoms. Allergy to latex is uncommon in the general population, and reports of mild allergic reactions to condoms are very rare. Severe allergic reactions to condoms are extremely rare. Plastic condoms made of synthetic materials offer an alternative for individuals who are allergic or sensitive to latex. Plastic condoms are expected to provide the same protection as latex condoms, but they have not been studied as thoroughly. The United States Food and Drug Administration recommends that condoms made of plastic be used for protection from STIs, including HIV, only if a person cannot use latex condoms. Condoms made of animal skin such as lambskin (also called natural skin condoms) are not effective for preventing STIs, including HIV, however. Myth: Premature ejaculation Some people incorrectly believe that external condoms constrict an erect penis, causing premature ejaculation. Fact: Using an external condom does not cause premature ejaculation. On the contrary, condoms can help users maintain an erection longer and prevent premature ejaculation, especially when the placement of the condom on the penis is a routine part of sexual foreplay. Myth: Promiscuity Some people believe that external condoms encourage infidelity, promiscuity, or prostitution. Fact: There is no evidence that condoms or other methods of contraception affect behavior. The evidence on contraception in general shows that sexual behavior is unrelated to contraceptive use. In fact, using contraception shows responsible behavior in order to avoid unintended pregnancy and sexually transmitted infections. Myth: Sexual Desire and sexual pleasure Some people incorrectly believe that condom use decreases a man’s libido and can cause impotence or that condoms reduce or interfere with sexual pleasure. Fact: There is no evidence to suggest that condom use causes impotence. Impotence has many causes. Some causes are physical, some are emotional. Condoms themselves do not cause impotence. A few men may have problems keeping an erection when using condoms, however. Other men, especially older men, may have difficulty keeping an erection because condoms can dull the sensation of having sex. Using more lubrication may help increase sensation for men using condoms. Some couples become frustrated and lose some of their sexual excitement when they stop to put on a condom. Some men and women complain that the condom dulls sensation. However, many couples learn to enjoy using condoms as part of their sexual foreplay. In fact, many women and men often say they have better sex when they use condoms, because they can focus on their sexual pleasure without the worry about unintended pregnancy and sexually transmitted infections (STIs). A couple may wish to use either a textured, ultra thin, or transparent condom to increase stimulation. Pleasure may also be increased by lubricating the inside and outside of the condom with water-based lubricants. A drop or two of lubricant on the inside of the condom before it is unrolled can help increase the sensation of sex for some men. Too much lubricant inside, however, can make the condom slip off. Lubricants made of glycerine or silicone are safe to use with latex condoms. Clean water and saliva also can be used for lubrication. Do not use products made with oil as lubricants for latex condoms as they can damage latex. External condom use does not interfere with sexual pleasure if the time when you use the condom during intercourse is correct. (Malaysia) If you use condoms correctly they do not interfere with sexual pleasure. (Lithuania) This is not true, please practice using condoms and get experience. (Bangladesh) When using a condom, you forget that you have a condom on your penis. Focus on what you are doing and you will get the same enjoyment. (St. Lucia) External condoms doenot influence the man’s libido or interfere with pleasure. You can use condoms and have the same pleasure. (Central Africa Republic) Myth: Size of penis Some people believe incorrectly that men who have a large penis will not be able to find an external condom that fits them properly. Fact: There are many different kinds and brands of condoms that vary in features such as shape, size, color, lubrication, thickness, texture, and whether or not they are coated with spermicide. Although there are considerable variations between the sizes of individual penises, there is no established market of different sized condoms, even in developed countries. Users should be advised to try different brands to find out which fits best. Condoms of 49mm width are readily available and are the preferred size for a smaller condom. Although there is no “standard” size for larger condoms, some manufacturers produce condoms of 56mm width. Myth: Who can use the method Some people do not want to use external condoms because they incorrectly believe that they should be used only by people in casual relationships, people who have extra marital sexual relations, or by people who have sex for money. Fact: Condoms are an appropriate contraceptive method for anyone, regardless of marital status or sexual behavior, and should be provided to all individuals who request them. While many casual partners rely on condoms for STI protection, married couples all over the world use condoms for pregnancy protection too.
12 October 2012
Exploring new territories: dialogues on comprehensive sexuality education
Exploring new territories report captures new and critical thinking about comprehensive sexuality education (CSE) sets out different pedagogical (teaching and learning) approaches identifies new priorities for CSE recognises the challenges CSE presents asks what else we need to research and discover "Comprehensive sexuality education should respond to and celebrate the diversity that exists among young people across the world. It should equip young people with knowledge, skills, attitudes and values to determine and enjoy their sexuality. Comprehensive sexuality education should take a positive and respectful approach to sexuality and sexual relationships, and be part of broader emotional and social development providing opportunities to acquire life skills and nurture personal values." This document captures a discussion designed to generate critical thinking about CSE: moving beyond developing curricula and activities to thinking about delivery and different pedagogical (teaching and learning approaches); moving beyond providing knowledge to developing skills; moving beyond public health outcomes and towards human rights and gender equality; and how to measure success. A snapshot of the challenges identified: balancing broader rights and gender equality outcomes with specific public health outcomes ensuring appropriateness in different contexts applying evidence-based approaches to both content and method pre-empting and managing resistance to new approaches What else we need to know – new areas for research developing and testing new indicators for the effectiveness and impact of CSE examining how best to foster high quality rights-based teaching and learning skills how to develop effective and continuous communication with parents and community leaders the best strategies to link CSE with health and social service provision for young people Includes: a table of ‘challenges’ ‘opportunities’ and ‘recommendations’ key questions and issues explored during the workshop a checklist of values that underpin CSE a resource list
06 July 2012
Annual Performance Report 2011-12
2012 is IPPF’s 60th year. The Annual Performance Report confirms, once again, IPPF’s vital role in human development. It opens with an overview of the external challenges that threaten sexual and reproductive health and rights (SRHR). Despite these challenges, IPPF continues to deliver impressive results. In 2011, Member Associations contributed to 116 policy and/or legislative changes in support or defence of sexual and reproductive health and rights (SRHR). The Federation as a whole provided 89.6 million SRH services with the majority going to the poor and vulnerable, including young people. Robust systems and processes have ensured that money has been invested cost-effectively where it is most needed.
12 June 2012
At a Glance 2010
Key facts and figures highlighting IPPF's achievements in 2009. Sexual and reproductive ill health causes over 30% of the global burden of disease among women of childbearing age and without IPPF, this burden would be even greater.
29 May 2012
IPPF Strategic Framework: 2005 - 2015
The product of a Federation-wide consensus, this framework brings together the ideas and experience of IPPF Member Associations, senior volunteers, Regional Offices and Central Office, and has been approved by the Governing Council. By combining an understanding of our past with a vision for our future, this new plan presents a 'framework of opportunity' that Member Associations can interpret to develop the most appropriate response to specific sexual and reproductive health challenges. The ‘Strategic Framework’ is not intended to impose a rigid set of rules or constraints. Rather, it embraces the diversity of situations Member Associations and regions face. While providing this flexibility, the framework unites the Federation in a common vision on which we are compelled to act if we are to meet the needs of women, men and young people throughout the world.
10 May 2012
Included Involved Inspired: A Framework for Youth Peer Education Programmes
The Included, involved, inspired framework promotes the benefits of youth participation through peer education guides us through planning, preparation, implementation and evaluation describes best practice provides tools to support the process of managing peer education places young people at the centre of all the processes "Peer education should support young people – both the peer educators themselves and those receiving information and services – to exercise their rights to sexual health, diversity and choice. We see peer educators as more than simply agents for behavioural change in themselves and their peers – our programmes show a commitment to also empowering them as individuals. In other words, a rights-based approach to peer education helps young people to develop the SRH knowledge, skills and attitudes needed to make their own choices regarding their sexuality and health." Peer education makes young people real stakeholders, addresses discrimination, and improves access to services. Participation means altering the power balance between young people and adults; enabling young people to identify their own problems; and ensuring that young people in all their diversity are involved in programme activities. This framework for programme designers, managers and co-ordinators, supervisors, trainers and young people can be used alongside existing guidelines and training materials to ensure peer education programmes are effective and empowering. It covers 10 stages of a peer education programme with detailed information on: Planning a peer education programme Selecting programme managers and coordinators Recruiting peer educators Training peer educators Implementing programmes: involving young people at every stage and in different roles Developing content Providing materials and condoms Supporting and keeping peer educators motivated Linking to services Monitoring, evaluation and document of programmes Includes: case studies from Nepal, the Dominican Republic, Colombia, Brazil, Sri Lanka, Peru, Guatemala, Kenya, India a check list of suggested qualities to look for, and to discuss with, a potential peer educator a check list of what makes a good training programme a case study on involving young people in monitoring and evaluation a definition of key terms a graphic of Olsson’s adapted ‘stairs of tolerance’ checklist of rules and responsibilities of a peer educator and peer counsellor 13 forms and tools for peer education programmes information on IPPF youth policies a list of peer education resources and websites
10 May 2012
From Evidence to Action: Advocating for comprehensive sexuality education
From evidence to action: advocating for comprehensive sexuality education defines CSE, answers common questions and sorts fact from fiction connects good quality CSE to global health goals promotes approaches which recognise young people’s lived experience links to reports on what works and what obstructs CSE and SRHR goals provides a checklist of activities for CSE advocates "Good sexuality education is essential to help young people to prepare for healthy and fulfilling lives. High quality information and comprehensive sexuality education can equip them with the knowledge, skills and attitudes they need to make informed choices now and in the future; to enhance their independence and self-esteem; and to help them to experience their sexuality and relationships in a positive and pleasurable way." There is evidence that CSE is effective and that abstinence-only approaches are ineffective. Evidence can provide the basis for promoting new thinking, and changing national approaches to teaching by demonstrating that a rights-based approach is a highly successful teaching methodology. It answers these questions: What is CSE? Why do it? What should it include? How can we deliver it? How can we advocate for it? This resource can help develop a greater understanding of IPPF’s vision for rights-based CSE; provide the evidence base for CSE, identifying successful characteristics, approaches and outcomes; support advocacy work with practical advice on creating the climate for CSE programmes; respond to challenges and difficult questions on comprehensive sexuality education from members of the community, addressing opposition and resistance; and create a better understanding of the links between comprehensive sexuality education and HIV prevention, human rights, health outcomes and global health goals. Young people need a realistic approach to their sexual and reproductive health: looking at psychological, socio-cultural and ethical dimensions and beyond the simply biological. CSE programmes should be rights-based; address gender and pleasure; provide choice; develop critical thinking skills; and reach vulnerable and marginalised groups. Includes: a checklist of activities to advocate for CSE ways in which comprehensive sexuality education helps further global health goals including gender equality, maternal health and combating HIV/AIDS international human rights conventions and documents that support the case for CSE links to HIV prevention a reading list of research and briefings on CSE answers to a range of common questions and myths about young people, sexual health and sexuality education answers to questions about the how, when, where and what of sexuality education A checklist of activities to advocate for comprehensive sexuality education p.16
03 May 2012
IPPF Sexual Rights Declaration Pocket Guide
02 May 2012
Sexual Rights: An IPPF declaration (abridged)
The IPPF declaration is grounded in and informed by international agreements such as United Nations Conventions. This abridged version to be used in conjunction with IPPF's original Sexual Rights Declaration.
19 April 2012
Participate: The voice of young people in programmes and policies
This is part of the Inspire pack of resources on young people's sexual and reproductive health services and programmes, for health providers and practitioners.
11 March 2019
Myths and facts about external condoms
This page was originally published in 2012 and has since been updated. External condoms (sometimes referred to as 'male' condoms) are placed over an erect penis. Learn how to put one on and find out about internal condoms. Back to external condoms – join us as we bust some common myths about this popular contraceptive method. Myth: Complications with method Some clients who seek family planning incorrectly believe that external condoms can easily get lost in a vagina or uterus and can travel through a woman’s body, requiring surgery to get the condom out. Fact: Studies indicate that a condom rarely slips off completely during intercourse. On average, about 2% of condoms break or slip off completely during sex, primarily because they are used incorrectly. Slippage during withdrawal can be minimized if the rim of the condom is held against the base of the penis during withdrawal after ejaculation. However, if a condom does slip, it will go no further than the woman’s vagina, where it can be easily retrieved, with no need for surgery. If a man notices a break or slip, he should tell his partner so that she can use emergency contraceptive pills if she wants. Myth: Effectiveness Some people who seek family planning do not want to use external condoms because they incorrectly believe that condoms are not effective in preventing pregnancy or sexually transmitted infections, including HIV. Fact: The external condom is a sheath, or covering, that fits over an erect penis. It works by forming a barrier that keeps sperm out of the vagina, preventing pregnancy. It also keeps infections that are in semen, on the penis, or in the vagina from infecting the other partner. It is usually made of very thin latex rubber, although a minority are made of either animal tissue or polyurethane (plastic). Condoms are the only contraceptive method that can protect against both pregnancy and sexually transmitted infections (STIs), including HIV transmission, when used for vaginal, oral, or anal sex. In order for condoms to be most effective they must be used correctly and consistently (with every act of sex). The risk of pregnancy or contracting sexually transmitted infections is greatest when condoms are not used correctly with every act of sex. When used correctly and consistently, condoms are 98% effective in preventing pregnancy. This means that when used consistently and correctly, about 2 of every 100 women whose partners use condoms become pregnant over the first year of use. Condoms do not have holes that HIV can pass through. In fact, when used consistently and correctly, condom use prevents 80% to 95% of HIV transmission that would have occurred without condoms. Plastic condoms are expected to provide the same protection as latex condoms, but they have not been studied thoroughly. Condoms made from animal membrane DO NOT protect against HIV and other STIs. On average, about 2% of condoms break or slip off completely during sex, primarily because they are used incorrectly. Used properly, condoms seldom break. Lubrication helps avoid condom breakage. There are three ways to provide lubrication—natural vaginal secretions, adding a lubricant, or using condoms packaged with lubricant on them. Sometimes lubricants made of glycerine or silicone, which are safe to use with latex condoms, are available. Clean water and saliva also can be used for lubrication. Do not use products made with oil as they can damage latex condoms. QUICK POLL: Are external condoms your contraceptive of choice?YesNo Myth: Health risks and side effects Some people incorrectly believe that using external condoms can cause side effects or health risks such as illness, infection, disease, or cancer. Fact: There are no known serious short or long term side effects associated with the use of condoms. When a condom is used, ejaculation occurs as normal, so there is no sperm “back up.” There is no evidence that condoms cause cancer, either in men or women. In fact, the use of condoms may help protect against conditions caused by STIs including recurring pelvic inflammatory disease, cervical cancer, and infertility. It is possible that a person may experience mild irritation in or around the vagina or penis or mild allergic reaction to a condom (itching, redness, rash, and/or swelling of genitals, groin, or thighs during or after condom use). Severe allergic reactions involve hives or rash over much of the body, dizziness, difficulty breathing, or loss of consciousness after coming in contact with latex. Both men and women can be allergic to latex and latex condoms. Allergy to latex is uncommon in the general population, and reports of mild allergic reactions to condoms are very rare. Severe allergic reactions to condoms are extremely rare. Plastic condoms made of synthetic materials offer an alternative for individuals who are allergic or sensitive to latex. Plastic condoms are expected to provide the same protection as latex condoms, but they have not been studied as thoroughly. The United States Food and Drug Administration recommends that condoms made of plastic be used for protection from STIs, including HIV, only if a person cannot use latex condoms. Condoms made of animal skin such as lambskin (also called natural skin condoms) are not effective for preventing STIs, including HIV, however. Myth: Premature ejaculation Some people incorrectly believe that external condoms constrict an erect penis, causing premature ejaculation. Fact: Using an external condom does not cause premature ejaculation. On the contrary, condoms can help users maintain an erection longer and prevent premature ejaculation, especially when the placement of the condom on the penis is a routine part of sexual foreplay. Myth: Promiscuity Some people believe that external condoms encourage infidelity, promiscuity, or prostitution. Fact: There is no evidence that condoms or other methods of contraception affect behavior. The evidence on contraception in general shows that sexual behavior is unrelated to contraceptive use. In fact, using contraception shows responsible behavior in order to avoid unintended pregnancy and sexually transmitted infections. Myth: Sexual Desire and sexual pleasure Some people incorrectly believe that condom use decreases a man’s libido and can cause impotence or that condoms reduce or interfere with sexual pleasure. Fact: There is no evidence to suggest that condom use causes impotence. Impotence has many causes. Some causes are physical, some are emotional. Condoms themselves do not cause impotence. A few men may have problems keeping an erection when using condoms, however. Other men, especially older men, may have difficulty keeping an erection because condoms can dull the sensation of having sex. Using more lubrication may help increase sensation for men using condoms. Some couples become frustrated and lose some of their sexual excitement when they stop to put on a condom. Some men and women complain that the condom dulls sensation. However, many couples learn to enjoy using condoms as part of their sexual foreplay. In fact, many women and men often say they have better sex when they use condoms, because they can focus on their sexual pleasure without the worry about unintended pregnancy and sexually transmitted infections (STIs). A couple may wish to use either a textured, ultra thin, or transparent condom to increase stimulation. Pleasure may also be increased by lubricating the inside and outside of the condom with water-based lubricants. A drop or two of lubricant on the inside of the condom before it is unrolled can help increase the sensation of sex for some men. Too much lubricant inside, however, can make the condom slip off. Lubricants made of glycerine or silicone are safe to use with latex condoms. Clean water and saliva also can be used for lubrication. Do not use products made with oil as lubricants for latex condoms as they can damage latex. External condom use does not interfere with sexual pleasure if the time when you use the condom during intercourse is correct. (Malaysia) If you use condoms correctly they do not interfere with sexual pleasure. (Lithuania) This is not true, please practice using condoms and get experience. (Bangladesh) When using a condom, you forget that you have a condom on your penis. Focus on what you are doing and you will get the same enjoyment. (St. Lucia) External condoms doenot influence the man’s libido or interfere with pleasure. You can use condoms and have the same pleasure. (Central Africa Republic) Myth: Size of penis Some people believe incorrectly that men who have a large penis will not be able to find an external condom that fits them properly. Fact: There are many different kinds and brands of condoms that vary in features such as shape, size, color, lubrication, thickness, texture, and whether or not they are coated with spermicide. Although there are considerable variations between the sizes of individual penises, there is no established market of different sized condoms, even in developed countries. Users should be advised to try different brands to find out which fits best. Condoms of 49mm width are readily available and are the preferred size for a smaller condom. Although there is no “standard” size for larger condoms, some manufacturers produce condoms of 56mm width. Myth: Who can use the method Some people do not want to use external condoms because they incorrectly believe that they should be used only by people in casual relationships, people who have extra marital sexual relations, or by people who have sex for money. Fact: Condoms are an appropriate contraceptive method for anyone, regardless of marital status or sexual behavior, and should be provided to all individuals who request them. While many casual partners rely on condoms for STI protection, married couples all over the world use condoms for pregnancy protection too.