



One of our main priorities is to ensure universal access to, and informed use of effective contraception. Millions of people lack the knowledge and information to determine when or whether they have children, and they are unable to protect themselves against sexually transmitted infections (STIs).
Articles about Contraception

11 March 2019
Myths and facts about implants
This page was originally published in 2012 and has since been updated. Contraceptive implants are thin, small (4cm), flexible rods which are implanted under the skin of the upper arm by a doctor or a nurse. They are 99% effective in preventing pregnancy. The implant rods contain progestins which are steadily released into the woman’s bloodstream. Progestins are like the hormone progesterone, which is produced naturally within a woman’s body. The continuous release of progestins stops a woman releasing an egg every month (ovulation), and thickens the mucus from the cervix (neck of the womb), making it difficult for sperm to pass through to the womb and reach an unfertilized egg. Implants protect against pregnancy soon after as they have been inserted. Depending on the type of implant, they last between 3-5 years, but can be removed at any time. Fertility returns when the implant is removed. Some women experience side effects form implants. It is common, but not harmful, to experience changes in menstrual bleeding patterns. Other possible side effects include abdominal pain, headaches, breast tenderness and acne. Side-effects often diminish over time, especially after the first few months to a year of use, but if you are concerned about side effects, you should go and talk to your provider. When fitting the implant, a local anaesthetic is used to numb the area. It makes a small wound in the arm, which is closed with a dressing and does not need stitches. Contraceptive implants do NOT protect against sexually transmitted infections (STIs, including HIV). To protect against STIs, male or female condoms need to be used. Myth: Pregnant while using an implant Some women who seek family planning believe that implants will interrupt an existing pregnancy. Fact: A fetus will not be harmed by the insertion of an implant Implants work primarily by thickening cervical mucus, which blocks sperm from meeting an egg, and by disrupting the menstrual cycle and preventing ovulation. Implants do not interrupt pregnancy. Good evidence shows that implants will not affect the pregnancy or harm the fetus if a woman is already pregnant when implants are inserted or becomes pregnant while using implants. Myth: Getting an implant is painful and could cause infection Some women who seek family planning believe that the insertion of implants requires surgery or that insertion is painful and causes infection. They may also have misconceptions about the removal of implants. Fact: No stitches, no noticeable scar, and it can be removed at any time Health professionals with specific training perform a minor surgical procedure to insert implants. The provider gives the patient an injection of local anesthetic under the skin of her arm to prevent pain while the implants are inserted. This injection may sting. The woman remains fully awake during the procedure. Insertion takes an average of 4 to 5 minutes for Norplant, 2.5 minutes for Jadelle, and 1.5 minutes for Implanon. Insertion can take more or less time, depending on the skill of the provider. The incision is small and stitches are not required. In most cases, insertion does not leave a noticeable scar. Once inserted, the outline of the implants underneath the skin can be felt and sometimes seen. The woman may have bruising and feel pain or soreness for a few days afterward. Infection at the insertion site can occur, but is uncommon. When infection occurs, it is usually within the first two months after insertion. In rare cases, implants may start to come out of the skin. When this occurs, it is usually due to improper insertion or infection. A woman can have her implants removed at any time. Similar to insertion, implant removal is done by a specifically trained provider using local anesthesia and does not require stitches. Removal takes an average of 10 to 15 minutes for Norplant, 5 to 8 minutes for Jadelle, and 3 minutes for Implanon. Removal can take more or less time, depending on the skill of the provider. Difficulties with removal are rare if the implants were properly inserted and the provider is skilled. POLL: Have you tried the implant as a method of contraception?(Please only answer this question if you have the potential to get pregnant. This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)Yes – I currently have one!I used to have one, but not anymoreI've never had an implant Myth: Health risks and side effects Some women who seek family planning do not want to use implants because they have misconceptions about implants causing illness or problems such as cancer, blindness, or birth defects. Fact: Implants have several known health benefits In addition to changes in menstrual bleeding, the most common side effects of implants are headaches, abdominal pain, and breast tenderness. These side effects are not an indication of illness and usually lessen or go away within the first year of use. Studies have not shown increased risk of cancer, blindness or birth defects with the use of implants. They have been shown to greatly reduce the risk of ectopic pregnancy and protect against symptomatic pelvic inflammatory disease. Implants may also help protect against iron-deficiency anemia. Myth: Complications with method Some women who seek family planning believe that implants can cause complications in the arm in which they are inserted or that they can travel from the insertion site to other parts of the body. Fact: Implants cannot travel to other parts of the body They remain where they are inserted until they are removed. In rare cases, a rod may start to come out of the skin, usually during the first four months since insertion. This typically happens because the implants were not inserted well or because of an infection at the insertion site. If expulsion occurs, the woman should return to the clinic as soon as possible and use a back-up family planning method in the meantime. Providers can replace the rods. Myth: Infertility and ectopic pregnancy Some women who seek family planning believe that using implants will cause infertility, delay the return of fertility after the implants are removed, or cause ectopic pregnancies (pregnancy in which the fertilized egg implants in tissue outside the uterus). Fact: Implant doesn't affect your fertility, and reduces the risk of ectopic pregnancy Implants stop working once they are removed and their hormones do not remain in the woman’s body. Implant use does not affect a woman’s ability to become pregnant, although fertility decreases with a woman’s age. One major study found that women who have had their implants removed can become pregnant as quickly as women who have stopped using nonhormonal methods. Implants substantially reduce the risk of ectopic pregnancy. In the United States, the rate of ectopic pregnancy among women who are not using a contraceptive method is 650 ectopic pregnancies per 100,000 women per year. The rate of ectopic pregnancy among women using implants is 6 ectopic pregnancies per 100,000 women per year. Even in the very rare cases when implants fail and pregnancy occurs, the great majority of these pregnancies are not ectopic. Only 10 to 17 of every 100 pregnancies due to the failure of implants are ectopic. Myth: Who can use the method Some women who seek family planning believe that implants should not be used by women who are young or who have not had children. Fact: Nearly all women can use implants safely and effectively Implants are suitable for women of any age, regardless of whether they have had children or not. Implants do not make women infertile—fertility returns as soon as implants are removed. Breastfeeding women can use implants if at least six weeks have passed since they have given birth. Implants may not be suitable for women who require a family planning method without hormones. For example, women who have or have had breast cancer and women with active, serious liver disease should choose an alternative method. Myth: Menstrual bleeding Some women who seek family planning incorrectly believe that using implants will cause harmful changes to menstrual bleeding. Fact: Changes may occur, but generally they are not harmful Changes in menstrual bleeding commonly occur with implant use, but some women do not experience any change. Typically, changes in bleeding patterns are more dramatic during the first year of use and either lessen or stop after the first year. Prolonged or heavy bleeding (lasting over eight days or generating twice as much blood as normal) due to implants generally is not harmful. Menstruation may also cease after one or two years of implant use, which is not harmful either—blood will not build up inside the woman. Myth: Sexual pleasure Some women who seek family planning believe that implants will reduce a woman’s libido or affect a couple’s sexual life in some way. Fact: No evidence to suggest that implants can reduce a woman’s libido There is no evidence to suggest that implants can reduce a woman’s libido. Some women using implants report negative changes in mood and sex drive, while some report improved mood and sex drive. Such changes could be caused by many other factors, so it is difficult to attribute them to implant use. A large majority of implant users do not report any change.
12 June 2012
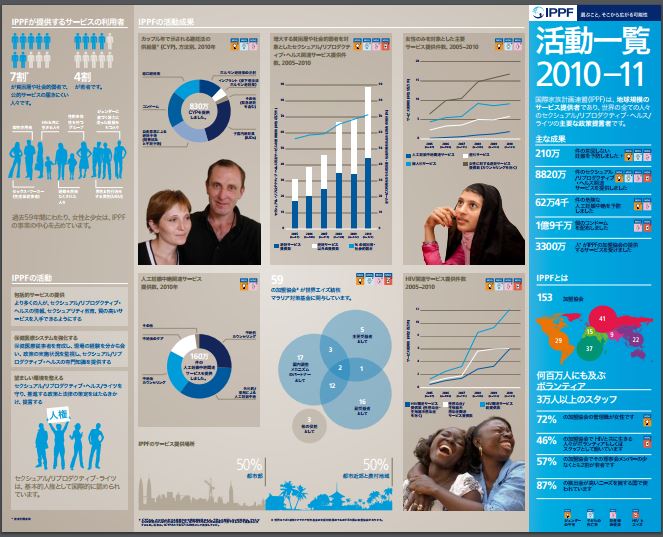
At a Glance 2010
Key facts and figures highlighting IPPF's achievements in 2009. Sexual and reproductive ill health causes over 30% of the global burden of disease among women of childbearing age and without IPPF, this burden would be even greater.
29 May 2012
IPPF Strategic Framework: 2005 - 2015
The product of a Federation-wide consensus, this framework brings together the ideas and experience of IPPF Member Associations, senior volunteers, Regional Offices and Central Office, and has been approved by the Governing Council. By combining an understanding of our past with a vision for our future, this new plan presents a 'framework of opportunity' that Member Associations can interpret to develop the most appropriate response to specific sexual and reproductive health challenges. The ‘Strategic Framework’ is not intended to impose a rigid set of rules or constraints. Rather, it embraces the diversity of situations Member Associations and regions face. While providing this flexibility, the framework unites the Federation in a common vision on which we are compelled to act if we are to meet the needs of women, men and young people throughout the world.

03 May 2012
IPPF Sexual Rights Declaration Pocket Guide
02 May 2012
Sexual Rights: An IPPF declaration (abridged)
The IPPF declaration is grounded in and informed by international agreements such as United Nations Conventions. This abridged version to be used in conjunction with IPPF's original Sexual Rights Declaration.

11 March 2019
Myths and facts about the Pill
This page was originally published in 2012 and has since been updated. Oral contraceptives (the Pill) are hormonally active pills which are usually taken by women on a daily basis. They contain either two hormones combined (progestogen and estrogen) or a single hormone (progestogen). Combined oral contraceptives suppress ovulation. Progestogen-only contraceptives also suppress ovulation in about half of women (they are slightly less effective). Both types cause a thickening of the cervical mucus, blocking sperm penetration. Oral contraceptives are 92 - 99% effective. A woman can decide to start taking the pill if she is sexually active or planning to become sexually active and is certain she is not pregnant. Some pills are taken daily for 21 days and stopped for 7 days before starting a new package. Other kinds are taken continuously for 28-day cycles. Oral contraceptives should be taken in order, at a convenient and consistent time each day. They are appropriate for women who are willing to use a method that requires action daily and who will be able to obtain supplies on a continuous basis. The pill offers continuous protection against pregnancy, it produces regular and shorter periods (and frequently a decrease in menstrual cramps), and it protects against ovarian and endometrial cancer, ectopic pregnancies and infections of the fallopian tubes. Possible side effects include nausea, breast tenderness, mild headaches, weight gain or loss. Very rarely, it can lead to serious health risks (e.g. blood clots, heart attack, and stroke). Risks are higher for women over 35 years who smoke. The pill does NOT protect against sexually transmitted infections (STIs, including HIV). To protect against STIs, a male or female condom must be used. POLL: Is the Pill your main method of contraception?(Please only answer this question if you have the potential to get pregnant. This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)Yes, I use it at the moment!I used to use it, but not anymoreNo, I've never used it Myth: There is a risk of birth defects Some women who seek family planning incorrectly believe that using COCs will cause birth defects in their babies. Fact: Good evidence shows that COCs will not cause birth defects and will not otherwise harm the fetus if a woman becomes pregnant while taking COCs or accidentally starts to take COCs when she already pregnant. Myth: The contraceptive pill can cause cancer Some women who seek family planning believe that combined oral contraceptives (COCs) cause cancers such as breast cancer, uterine cancer, and ovarian cancer. Fact: The use of combined oral contraceptives (COCs) is proven to decrease the risk of two gynecological cancers (ovarian and endometrial). It is difficult to know the effect of COC use on breast cancer and cervical cancer. The possibly increased risks that have been recorded in some studies are not large enough to outweigh benefits or to change current practice. Use of COCs helps protect women from two kinds of cancers—cancer of the ovaries and cancer of the lining of the uterus (endometrial cancer). This protection continues for 15 or more years after stopping use. Breast cancer Research findings about COCs and breast cancer are difficult to interpret. In studies, breast cancer is slightly more common among women using COCs and those who have used COCs in the past 10 years than among other women. Scientists do not know whether or not COCs actually caused the slight increase in breast cancers. It is possible that the cancers were already there before COC use but were found sooner in COC users. Both COC users and women who do not use COCs can have breast cancer. Cervical cancer Cervical cancer is caused by certain types of human papillomavirus (HPV). HPV is a common STI that usually clears on its own without treatment, but sometimes persists. Use of COCs for five years of more appears to speed up the development of persistent HPV infection into cervical cancer. The number of cervical cancers associated with COC use is thought to be very small. If cervical screening is available, providers can advise COC users—and all other women—to be screened every three years (or as national guidelines recommend) to detect precancerous changes in the cervix, which can be removed. Myth: You will experience general health problems Some women believe that COCs cause hair loss (alopecia), asthma, and headaches. Fact: A woman may experience short term side affects associated with use of combined oral contraceptive (COCs), including changes in bleeding patterns, headaches, and nausea. However such side effects are not a sign of illness, and usually stop within the first few months of using COCs. For a woman whose side effects persist, give her a different COC formulation. In women who are otherwise well, COC use may be continued for many years as there are no adverse effects related to long-term use. In fact, there are also long-term non-contraceptive health benefits of using COCs as they: Help protect against cancer of the lining of the uterus (endometrial cancer) Help protect against cancer of the ovaries Help protect against symptomatic pelvic inflammatory disease May help protect against ovarian cysts May help protect against iron-deficiency anemia Reduce menstrual cramps Reduce menstrual bleeding problems Reduce ovulation pain Reduce excess hair on face or body Reduce symptoms of polycystic ovarian syndrome Reduce symptoms of endometriosis Myth: There is confusion about how often and when to take the pill Some women who seek family planning are misinformed about how often or when they should take the pill. Fact: A woman can start using COCs any time she wants if she is reasonably certain that she is not pregnant. To be reasonably certain a client is not pregnant, providers can use the Pregnancy Checklist. If a client is starting her pack of pills within five days after the start of her menstrual period, there is no need for a backup method as she is immediately protected from pregnancy. If she starts COCs more than five days after the start of her menstrual period, she can start them any time it is reasonably certain she is not pregnant. She will need to use a "back up" method of contraception, such as a male or female condom, for the first seven days of taking pills to ensure protection from pregnancy. The effectiveness of oral contraception depends on a regular intake of the hormones contained in the pill. Therefore pills must be taken daily, until the pack is empty. Although the specific time of day does not matter, the pills should be taken at the same time every day to reduce side effects and to help women remember to take their pills more consistently. The client should be advised not to interrupt taking the pills before a pack is finished, even if she does not have sexual intercourse. If the pills are taken correctly, the client will always start a new pack on the same day of the week. If a client is taking pills from a 21-pill pack, she will wait seven days after taking the last pill in the pack before beginning a new pack. If a client is taking pills from a 28-pill pack, she will take the next pill from the next pack on the very next day. Women do not need to take a “rest” from COCs after taking them for a time. There is no evidence that taking a “rest” is helpful. In fact, taking a”rest” from COCs can lead to unintended pregnancy. COCs can safely be used for many years without having to stop taking them periodically. Myth: There is a risk of infertility, or a delayed return to fertility Women who seek family planning may incorrectly believe that using COCs will cause a long delay in conceiving or prevent them from being able to have children in the future. Fact: The combined oral contraceptive (COC) does not cause infertility. This is true regardless of how long a woman has taken the pill, the number of children the woman has had, or the age of the woman. In fact, some of the non-contraceptive benefits of the pill include preserving fertility by offering protection against pelvic inflammatory disease, endometriosis, and ectopic pregnancy. There is no evidence that COCs delay a woman's return to fertility after she stops taking them. Women who stop using COCs can become pregnant as quickly as women who stop using non-hormonal methods. Myth: Contraceptive pills can get absorbed into the wrong part of the body Many women who seek family planning incorrectly believe that COCs accumulate in the body and cause diseases and tumors, or get stored in the stomach, ovaries, or uterus and form stones. Fact: After the pills are swallowed, they dissolve in the digestive system, and the hormones they contain are absorbed into the bloodstream. After they produce their contraceptive effect, the hormones are metabolised in the liver and gut and are then eliminated from the body. They do not accumulate in the body anywhere. Myth: Contraceptive pills encourage 'promiscuity' Some clients who seek family planning wrongly believe that the pill encourages infidelity, promiscuity, or prostitution in women. Fact: There is no evidence that COCs affect women’s sexual behavior. The evidence on contraception in general shows that sexual behavior is unrelated to contraceptive use. In fact, using contraception shows responsible behavior in order to avoid unintended pregnancy and sexually transmitted infections. Myth: There will be an impact sexual desire and pleasure Some clients who seek family planning may believe that COCs reduce sexual pleasure or interest in sex (loss of libido) or that they cause frigidity in women. Fact: There is no evidence that COCs affect a woman's sex drive. Although some women using the pill have reported either an increase or decrease in sexual interest and performance, it is difficult to say whether such changes are a result of COCs or other life events. Myth: You will experience weight changes Some clients believe that COCs cause women to gain or lose weight. Fact: Most women do not gain or lose weight as a result of COC use. A woman's weight may fluctuate naturally due to changes in age or life circumstance. Because changes in weight are common, many women attribute their natural weight gain or loss to the use of COCs. Although a very small number of COC users may report weight change following COC use, studies have found that, on average, COCs do not affect weight. A few women experience sudden changes in weight when using COCs. These changes reverse after they stop taking COCs. It is not known why these women respond to COCs this way.

11 March 2019
Myths and facts about external condoms
This page was originally published in 2012 and has since been updated. External condoms (sometimes referred to as 'male' condoms) are placed over an erect penis. Learn how to put one on and find out about internal condoms. Back to external condoms – join us as we bust some common myths about this popular contraceptive method. Myth: Complications with method Some clients who seek family planning incorrectly believe that external condoms can easily get lost in a vagina or uterus and can travel through a woman’s body, requiring surgery to get the condom out. Fact: Studies indicate that a condom rarely slips off completely during intercourse. On average, about 2% of condoms break or slip off completely during sex, primarily because they are used incorrectly. Slippage during withdrawal can be minimized if the rim of the condom is held against the base of the penis during withdrawal after ejaculation. However, if a condom does slip, it will go no further than the woman’s vagina, where it can be easily retrieved, with no need for surgery. If a man notices a break or slip, he should tell his partner so that she can use emergency contraceptive pills if she wants. Myth: Effectiveness Some people who seek family planning do not want to use external condoms because they incorrectly believe that condoms are not effective in preventing pregnancy or sexually transmitted infections, including HIV. Fact: The external condom is a sheath, or covering, that fits over an erect penis. It works by forming a barrier that keeps sperm out of the vagina, preventing pregnancy. It also keeps infections that are in semen, on the penis, or in the vagina from infecting the other partner. It is usually made of very thin latex rubber, although a minority are made of either animal tissue or polyurethane (plastic). Condoms are the only contraceptive method that can protect against both pregnancy and sexually transmitted infections (STIs), including HIV transmission, when used for vaginal, oral, or anal sex. In order for condoms to be most effective they must be used correctly and consistently (with every act of sex). The risk of pregnancy or contracting sexually transmitted infections is greatest when condoms are not used correctly with every act of sex. When used correctly and consistently, condoms are 98% effective in preventing pregnancy. This means that when used consistently and correctly, about 2 of every 100 women whose partners use condoms become pregnant over the first year of use. Condoms do not have holes that HIV can pass through. In fact, when used consistently and correctly, condom use prevents 80% to 95% of HIV transmission that would have occurred without condoms. Plastic condoms are expected to provide the same protection as latex condoms, but they have not been studied thoroughly. Condoms made from animal membrane DO NOT protect against HIV and other STIs. On average, about 2% of condoms break or slip off completely during sex, primarily because they are used incorrectly. Used properly, condoms seldom break. Lubrication helps avoid condom breakage. There are three ways to provide lubrication—natural vaginal secretions, adding a lubricant, or using condoms packaged with lubricant on them. Sometimes lubricants made of glycerine or silicone, which are safe to use with latex condoms, are available. Clean water and saliva also can be used for lubrication. Do not use products made with oil as they can damage latex condoms. QUICK POLL: Are external condoms your contraceptive of choice?YesNo Myth: Health risks and side effects Some people incorrectly believe that using external condoms can cause side effects or health risks such as illness, infection, disease, or cancer. Fact: There are no known serious short or long term side effects associated with the use of condoms. When a condom is used, ejaculation occurs as normal, so there is no sperm “back up.” There is no evidence that condoms cause cancer, either in men or women. In fact, the use of condoms may help protect against conditions caused by STIs including recurring pelvic inflammatory disease, cervical cancer, and infertility. It is possible that a person may experience mild irritation in or around the vagina or penis or mild allergic reaction to a condom (itching, redness, rash, and/or swelling of genitals, groin, or thighs during or after condom use). Severe allergic reactions involve hives or rash over much of the body, dizziness, difficulty breathing, or loss of consciousness after coming in contact with latex. Both men and women can be allergic to latex and latex condoms. Allergy to latex is uncommon in the general population, and reports of mild allergic reactions to condoms are very rare. Severe allergic reactions to condoms are extremely rare. Plastic condoms made of synthetic materials offer an alternative for individuals who are allergic or sensitive to latex. Plastic condoms are expected to provide the same protection as latex condoms, but they have not been studied as thoroughly. The United States Food and Drug Administration recommends that condoms made of plastic be used for protection from STIs, including HIV, only if a person cannot use latex condoms. Condoms made of animal skin such as lambskin (also called natural skin condoms) are not effective for preventing STIs, including HIV, however. Myth: Premature ejaculation Some people incorrectly believe that external condoms constrict an erect penis, causing premature ejaculation. Fact: Using an external condom does not cause premature ejaculation. On the contrary, condoms can help users maintain an erection longer and prevent premature ejaculation, especially when the placement of the condom on the penis is a routine part of sexual foreplay. Myth: Promiscuity Some people believe that external condoms encourage infidelity, promiscuity, or prostitution. Fact: There is no evidence that condoms or other methods of contraception affect behavior. The evidence on contraception in general shows that sexual behavior is unrelated to contraceptive use. In fact, using contraception shows responsible behavior in order to avoid unintended pregnancy and sexually transmitted infections. Myth: Sexual Desire and sexual pleasure Some people incorrectly believe that condom use decreases a man’s libido and can cause impotence or that condoms reduce or interfere with sexual pleasure. Fact: There is no evidence to suggest that condom use causes impotence. Impotence has many causes. Some causes are physical, some are emotional. Condoms themselves do not cause impotence. A few men may have problems keeping an erection when using condoms, however. Other men, especially older men, may have difficulty keeping an erection because condoms can dull the sensation of having sex. Using more lubrication may help increase sensation for men using condoms. Some couples become frustrated and lose some of their sexual excitement when they stop to put on a condom. Some men and women complain that the condom dulls sensation. However, many couples learn to enjoy using condoms as part of their sexual foreplay. In fact, many women and men often say they have better sex when they use condoms, because they can focus on their sexual pleasure without the worry about unintended pregnancy and sexually transmitted infections (STIs). A couple may wish to use either a textured, ultra thin, or transparent condom to increase stimulation. Pleasure may also be increased by lubricating the inside and outside of the condom with water-based lubricants. A drop or two of lubricant on the inside of the condom before it is unrolled can help increase the sensation of sex for some men. Too much lubricant inside, however, can make the condom slip off. Lubricants made of glycerine or silicone are safe to use with latex condoms. Clean water and saliva also can be used for lubrication. Do not use products made with oil as lubricants for latex condoms as they can damage latex. External condom use does not interfere with sexual pleasure if the time when you use the condom during intercourse is correct. (Malaysia) If you use condoms correctly they do not interfere with sexual pleasure. (Lithuania) This is not true, please practice using condoms and get experience. (Bangladesh) When using a condom, you forget that you have a condom on your penis. Focus on what you are doing and you will get the same enjoyment. (St. Lucia) External condoms doenot influence the man’s libido or interfere with pleasure. You can use condoms and have the same pleasure. (Central Africa Republic) Myth: Size of penis Some people believe incorrectly that men who have a large penis will not be able to find an external condom that fits them properly. Fact: There are many different kinds and brands of condoms that vary in features such as shape, size, color, lubrication, thickness, texture, and whether or not they are coated with spermicide. Although there are considerable variations between the sizes of individual penises, there is no established market of different sized condoms, even in developed countries. Users should be advised to try different brands to find out which fits best. Condoms of 49mm width are readily available and are the preferred size for a smaller condom. Although there is no “standard” size for larger condoms, some manufacturers produce condoms of 56mm width. Myth: Who can use the method Some people do not want to use external condoms because they incorrectly believe that they should be used only by people in casual relationships, people who have extra marital sexual relations, or by people who have sex for money. Fact: Condoms are an appropriate contraceptive method for anyone, regardless of marital status or sexual behavior, and should be provided to all individuals who request them. While many casual partners rely on condoms for STI protection, married couples all over the world use condoms for pregnancy protection too.

11 March 2019
Myths and facts about the intra-uterine device (IUD)
This page was originally published in 2012 and has since been updated. Myth: Abortion Some couples do not want to use the IUD because they incorrectly believe that the IUD prevents pregnancy by causing abortions. Fact: IUDs do not work by causing abortions In the vast majority of cases, IUDs work by preventing fertilization. The copper-bearing IUD acts as a spermicide, killing or impairing sperm so they cannot reach the egg. IUDs that contain progestin cause the cervical mucus to thicken, which stops sperm from entering the uterus. Thus, the current evidence suggests that the main mechanisms of action of IUDs occur prior to fertilization. In very rare case, IUDs prevent implantation which is considered a contraceptive not an abortifacient effect. Myth: Effectiveness Some women do not want to use the IUD because they incorrectly believe that the IUD is not effective in preventing pregnancy or that the IUD loses its contraceptive effect after only a few years from the time of insertion. Fact: IUDs are the more than 99% effective! Both the hormonal and copper-bearing IUDs are highly effective contraceptive methods. In fact, they are among the most effective reversible methods, with pregnancy rates similar to those for female sterilization. Hormonal levonorgestrel-releasing IUD (LNG-IUD): Less than 1 pregnancy per 100 women using the LNG-IUD over the first year (2 per 1,000 women). That means the LNG-IUD will prevent pregnancy in 998 of 1,000 women. A small risk of pregnancy remains beyond the first year of use and continues as long as the woman is using the LNG-IUD. Over 5 years of LNG-IUD use, about 1 per 100 women (5 to 8 per 1,000 women) will become pregnant. The LNG-IUD is approved for up to 5 years of use. Copper-bearing IUDs: Less than 1 pregnancy per 100 women using an IUD over the first year (6 to 8 per 1,000 women). That means the IUD will prevent pregnancy for 992 to 994 of 1,000 women using IUDs will not become pregnant. A small risk of pregnancy remains beyond the first year of use and continues as long as the woman is using the IUD. Over 10 years of IUD use, about 2 per 100 women will become pregnant. The IUD is effective for up to 12 years. Myth: Health risks and side effects Some women do not want to use the IUD because they incorrectly believe that IUD causes side effects or health risks such as cancer, sexually transmitted infections, or birth defects. Fact: IUDs are safe! Infection related to IUD insertion probably occurs because the instruments or IUD carry with them organisms from the lower genital tract. If the organisms are bacteria normally present in the genital tract, then it seems that some mechanism automatically eliminates this contamination from the uterus soon after the insertion process without infection occurring. Risk of infection can be further reduced by following routine infection-prevention procedures including the “no-touch” insertion technique (not letting the loaded IUD or uterine sounds touch any unsterile surfaces such as hands, speculum, vaginal wall, or table top). The IUD never travels to the heart, brain, or any other part of the body outside the abdomen. The IUD normally stays within the uterus like a seed within a shell. Rarely, the IUD may come through (perforate) the wall of the uterus into the abdominal cavity. This is most often due to a mistake during insertion. Proper insertion technique can help prevent many problems, such as infection, expulsion, and perforation. If uterine perforation is suspected within 6 weeks after insertion or if it is suspected later and is causing symptoms, refer the client for evaluation to a clinician experienced at removing such IUDs. Usually, however, the out-of-place IUD causes no problems and should be left where it is. The woman will need another contraceptive method. POLL: Is an IUD your main method of contraception?(Please only answer this question if you have the potential to get pregnant. This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)Yes, I have one now!I used to have one, but not anymoreNo, I've never had one IUDs do not cause cancer in otherwise healthy women, but confirmed or suspected cancer of the genital tract is a contraindication to IUD use, because the increased risk of infection, perforation, and bleeding at insertion may make the condition worse. For the levonorgestrel-releasing IUD, breast cancer is also a contraindication. IUDs do not increase the risk of contracting STIs, including HIV. However, usually women who have a very high risk of exposure to gonorrhea or chlamydia should not have an IUD inserted. In special circumstances, when other, more appropriate methods are not available or acceptable to her, a qualified provider who can carefully assess a specific woman’s risk may decide that she can use an IUD. IUD use neither causes multiple pregnancies after removal nor increases the risk of birth defects, whether the pregnancy occurs with the IUD in place, or after removal. In the rare event that a client becomes pregnant with an IUD in situ, it is important to explain the risks of leaving the IUD in the uterus during pregnancy. There is a higher risk of preterm delivery or miscarriage, including infected (septic) miscarriage during the first or second trimester, which can be life-threatening. Early removal of the IUD reduces these risks, although the removal procedure itself involves a small risk of miscarriage. There is no evidence of increased risk of fetal malformations, however. Overall levels of Pelvic Inflammatory Disease (PID) in IUD users are low. A woman with chlamydia or gonorrhea at the time of IUD insertion, however, is at higher risk of PID in the first few weeks after insertion than she is later. After the first few weeks, an STI may be no more likely to progress to PID in an IUD user than for other women with STIs. To reduce the risk of infection during IUD insertion, providers can ensure appropriate insertion conditions, screening, and counseling, as well as regularly monitor and treat infection. Antibiotics are usually not routinely given before IUD insertion. Most recent research done where STIs are not common suggests that PID risk is low with or without antibiotics. When appropriate questions to screen for STI risk are asked and IUD insertion is done with proper infection-prevention procedures (including the no-touch insertion technique), there is little risk of infection. Antibiotics may be considered, however, in areas where STIs are common and STI screening is limited. If PID occurs or is suspected with an IUD in place, treatment should be started as soon as possible. There is no need to remove the IUD if a woman wants to continue using it. The PID should be treated and the IUD left in situ. If a woman wants it removed, it can be taken out after starting antibiotic treatment. An IUD should not be inserted in women who currently have a PID. It may be inserted as soon as she finishes treatment, if she is not at risk for reinfection before insertion. The copper in copper-bearing IUDs is not released into the blood. Levels of serum copper in long-term users of copper IUDs are similar to that of the normal population. Myth: Problems after removal Some couples do not want to use the IUD because they incorrectly believe that the IUD will cause infertility, ectopic pregnancy, or miscarriage. Fact: no increased risk of infertility Good studies find no increased risk of infertility among women who have used IUDs, including young women and women with no children. Whether or not a woman has an IUD, however, if she develops pelvic inflammatory disease (PID) and it is not treated, there is some chance that she will become infertile. PID can permanently damage the lining of the fallopian tubes and may partially or totally block one or both tubes enough to cause infertility. Fact: no increased risk of ectopic pregnancy or miscarriage after removal Because any pregnancy among IUD users is rare, ectopic pregnancy among IUD users is even rarer. An IUD does not increase a woman’s overall risk of ectopic pregnancy. In fact, an IUD user’s risk of an ectopic pregnancy is much lower than the risk to a woman who is not using any method of contraception. In the unlikely event of pregnancy in an IUD user, 6 to 8 in every 100 of these pregnancies is ectopic. Thus, the great majority of pregnancies after IUD failure are not ectopic. Still, ectopic pregnancy can be life-threatening, so a provider should be aware that ectopic pregnancy is possible if an IUD fails. IUDs do not cause miscarriages after they have been removed. If correct insertion technique is used, the use of an IUD will not cause any difficulty in future pregnancies. In the rare event that a client becomes pregnant with an IUD in situ, it is important to explain the risks of leaving the IUD in the uterus during pregnancy. There is a higher risk of preterm delivery or first- and second- trimester miscarriage, including infected (septic) miscarriage which can be life-threatening. Early removal of the IUD reduces these risks, although the removal procedure itself involves a small risk of miscarriage. If the client does not want to continue the pregnancy and if therapeutic termination of pregnancy is legally available, inform her accordingly. If she wishes to continue the pregnancy and the IUD strings are visible or can be retrieved safely from the cervical canal, gently remove the IUD or refer for removal. The client should return at once if she develops any signs of miscarriage or septic miscarriage (vaginal bleeding, cramping, pain, abnormal vaginal discharge, or fever). However, if the IUD strings cannot be found in the cervical canal and the IUD cannot be safely retrieved, refer for ultrasound, if possible, to determine whether the IUD is still in the uterus. If the IUD is still in the uterus, if ultrasound is not available, or if the client chooses to keep the IUD, her pregnancy should be followed closely by a nurse or doctor. She should see a nurse or doctor at once if she develops any signs of septic miscarriage. Myth: change of menstrual pattern Many couples do not want to use the IUD because they incorrectly believe that using the IUD will cause either no monthly bleeding (amenorrhea) or heavier, painful, and more frequent menstrual bleeding, and this is harmful for your system. Fact: change in bleeding patterns are not harmful Women can experience changes in bleeding patterns depending on the type of IUD. Women using copper-bearing IUDs may experience: Heavy and prolonged monthly bleeding Irregular bleeding More cramps and pain during monthly bleeding These bleeding changes are normal and usually are not signs of illness. They are most common in the first 3 to 6 months after insertion and usually lessen with time. A provider should evaluate for an underlying condition unrelated to method use if: Cramping continues and occurs between monthly bleeding; Heavy or prolonged bleeding continues, or if bleeding starts suddenly after several months of normal bleeding or long after the IUD was inserted, or; Irregular bleeding persists after 6 months, or starts suddenly after several months of normal bleeding. Severe anaemia requires careful consideration because if heavier menstrual periods are experienced, the additional monthly blood loss could worsen existing anaemia. The anaemia should be treated before an IUD is inserted. The LNG-IUD may actually help to reduce anaemia by reducing blood loss. Women using the LNG-IUD may experience heavy, prolonged, or irregular bleeding in the first few months, but then experience: Lighter, regular, and predictable bleeding Infrequent, light, or no monthly bleeding These bleeding changes also are normal and usually are not signs of illness. Copper-bearing IUDs rarely cause monthly bleeding to stop completely. However, women using an LNG-IUD may not experience monthly bleeding due to strong uniform suppression of the endometrium. If monthly bleeding does not occur while a woman is using a copper-bearing IUD, pregnancy should be excluded. If the woman is not pregnant, other causes of no monthly bleeding should be investigated. Pain associated with menstruation may increase in some women, but usually this is only for the first month or two. The LNG-IUD may reduce the pain associated with menstruation. Non-steroidal anti-inflammatory drugs may also reduce discomfort. Myth: Sexual desire and sexual pleasure Some couples do not want to use the IUD because they incorrectly believe that the IUD will cause inconvenience during sex, pain for the male partner because the strings will hurt the penis, or that using the IUD causes discomfort and pain for the woman during sex. Fact: It might make you more relaxed about unintended pregnancies and enjoy sex even more! There is no reason why an IUD should negatively affect sexual pleasure. On the contrary, being free from fear of pregnancy may allow both partners, especially the woman, to enjoy their sexual life. There is no reason why an IUD should cause discomfort or pain during sexual intercourse unless the woman is already having cramps, which sometimes occur during the first few weeks after insertion. Sexual intercourse cannot displace an IUD. Sometimes a man can feel the strings if they are too long. If this bothers him, cutting the strings shorter should solve the problem. Sometimes a man can also feel discomfort if the strings are cut too short. To remedy the problem, the provider can cut them even shorter so they are not coming out of the cervical canal. The woman should be told beforehand, however, that this will mean she may not be able to feel the strings to check her IUD, and removing her IUD may be more difficult. Alternatively, she can have the IUD replaced with a new one and the strings cut to the correct length. The strings should be cut so that 3 centimeters hang out of the cervix. A man may feel discomfort during sex if the IUD has started to come out through the cervix. If a woman suspects this, she should see a doctor or nurse immediately. Proper counselling of the male partner may be appropriate. Myth: Who can use the method Many women do not want to use the IUD because they incorrectly believe that the IUD should not be used by women who are young or who have not had children. Fact: IUDs are safe for a wide range of women There is no minimum or maximum age requirement for using the IUD. An IUD should be removed after menopause has occurred — at least 12 months after her last monthly bleeding. There is also no requirement that a woman must have children to use the IUD. A history of pelvic infection or multiple sex partners (one indication that a woman is at high risk for STIs) make the choice of an IUD inappropriate for such women. The myth that young women and women without children cannot use IUDs stems from fears about a higher risk of expulsion in these women and fears about a higher risk of infection in these women. Expulsion is more likely in certain circumstances, such as young age at insertion (under 20 or 25 years old). Some studies also have found a higher rate of expulsion among women who have no children. The additional risk of expulsion, however, is not sufficient to deny IUDs to women in these circumstances, because the advantages of the IUD outweigh the risks of expulsion. Women with current gonorrheal or chlamydial infection should not have an IUD inserted. Since laboratory STI tests usually are not available, World Health Organization guidance considers STI risk assessment and physical examination essential to safe use of IUDs, but not laboratory tests. Providers should not determine a woman’s STI risk based on her age or whether she has had children. Rather, the provider can discuss risky behaviors or situations in their communities that they think are most likely to expose women to STIs, for example having more than one sexual partner in the last three months without always using condoms. The client can think about whether such situations occurred recently (in the past 3 months or so).
11 March 2019
Myths and facts about female sterilization
This page was originally published in 2012 and has since been updated. Female sterilization is an effective form of contraception that permanently prevents a woman from becoming pregnant. Sterilization does NOT protect against sexually transmitted infections (STIs), including HIV. The operation involves cutting or blocking the fallopian tubes, which carry eggs from the ovaries to the womb. This prevents the eggs from reaching the sperm and becoming fertilized. It can be a fairly minor operation, with many women returning home the same day. In most cases, female sterilization is more than 99% effective, and all women can be sterilized. However, sterilization should only be considered by women who do not want any more children, or who do not want children at all. Once a woman is sterilized, it is very difficult to reverse the process. Couples often decide upon sterilization mutually, when they both feel they do not want any more children. If a couple decides upon sterilization as their preferred contraceptive method, either partner could be sterilized. If both options are acceptable, vasectomy is preferable. It is simpler, safer, easier and less expensive. Myth: Sterilization causes cancer Some clients incorrectly believe that female sterilization will cause women to develop cancer of the reproductive organs (uterus, cervix, or ovaries). Fact: Female sterilization does not increase the risk of cancer of the reproductive organs which are defined below. Very little research has been done to investigate the relationship between breast cancer and female sterilization, but so far there is no evidence of such a link. Myth: All of a woman's reproductive organs will be removed Some clients incorrectly believe that female sterilization involves the removal of some or all of a woman’s reproductive organs, including the vagina. Fact: During the sterilization procedure, the ovaries, uterus, and cervix are left in place. Only the fallopian tubes (the tubes which carry eggs from the ovaries to the uterus) are blocked or cut. The two most common surgical approaches are laparoscopy and minilaparotomy. POLL: Have you undergone female sterlisation as a method of contraception?(Please only answer this question if you have the potential to get pregnant. This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)YesNo Myth: There are health risks and side effects Some clients incorrectly believe that female sterilization leads to health risks or side effects such as hysterectomy, poor health, pain, changes in menstrual bleeding or hormonal imbalances. Fact: There are no documented medical side effects of female sterilization. The few complications that do occur during or following sterilization, such as infection or abscess of the wound, can generally be kept to a minimum if appropriate techniques are used and if the procedure if performed in an appropriate setting. Local anesthesia is best for female sterilization because it has lower risks of complications than use of general anesthesia. The risks are lowest when local anesthesia is used without sedatives. If sedatives are used, providers should closely monitor the woman’s vital signs, such as pulse rate and blood pressure throughout the procedure. Also, most research finds no major changes in menstrual bleeding patterns after female sterilization. Myth: Sterilization means a woman will no longer ovulate Some people incorrectly believe that female sterilization prevents pregnancy either by stopping ovulation or by killing a woman’s egg. Fact: Female sterilization does not stop ovulation or harm a woman’s egg in any way. An egg will still be released each month, but it will dissolve and be reabsorbed by the body. Myth: You will lose your sex drive Some clients incorrectly believe that female sterilization causes women to lose their sex drive or lose their sexual ability. Fact: After sterilization a woman will look and feel the same as before. There is no loss of sexual drive or interest after female sterilization. She can have sex the same as before. She may find that sex is more enjoyable because she does not have to worry about getting pregnant. Myth: You will experience weight changes Some clients incorrectly believe that female sterilization will cause women to lose weight or to gain weight or that female sterilization will disfigure a woman’s body. Fact: Sterilization does not cause any changes in weight, appetite, or appearance. However, older women are more likely to choose sterilization for contraception than younger women and most women gain weight as they age. Myth: Only certain women can undergo sterilization Some women avoid female sterilization because they incorrectly believe that only women of a certain age or who have a certain number of children can undergo female sterilization. Fact: All women can have female sterilization. No medical conditions prevent a woman from using female sterilization.

30 January 2018
Myths and facts about the withdrawal method
This page was originally published in 2012 and has since been updated. Withdrawal (also known as 'pulling out') is when the a penis is removed from a vagina before ejaculation. This prevents the semen from entering the vagina-owner's body. However, even if the penis is withdrawn before ejaculation, pre-ejaculate fluid may contain sperm cells that can cause pregnancy and it may also contain organisms that cause sexually transmitted infections (STIs), including HIV. Withdrawal is not recommended as a main method of contraception. It is dependent on the penis-owner, it requires great self-control, self-awareness and motivation, it may affect sexual pleasure, and it provides no protection against STIs. People are advised to use withdrawal only if both partners are prepared to deal with the consequences of a pregnancy. Blog: Learn more about pre-ejaculatory fluid and if it can cause pregnancy Myth: Correct method use Some people have misconceptions about how to use withdrawal correctly. For example, people incorrectly believe that the clear fluid that comes out of a penis before ejaculation (pre-ejaculate fluid) can cause pregnancy. Fact: As the pre-ejaculate leaves the body, however, it may pick up sperm from a previous ejaculation that remains in the urethra. One study found small clumps of sperm in the pre-ejaculate fluid of some participants. Though only a few hundred sperm were present, they could theoretically pose a low risk of pregnancy. POLL: Have you ever tried withdrawal as a method of contraception?(This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)Yes – I do it all the timeYes, I've tried it but don't use it regularlyNo, never! Such small amounts of sperm can likely be flushed out with urination, although no research has verified this. If a person using withdrawal has ejaculated recently, they should urinate and wipe the tip of their penis to remove any remaining sperm before having sex again. Myth: Effectiveness Some people have misconceptions about the effectiveness of withdrawal. Fact: Withdrawal is one of the least effective contraceptive methods - although it offers better pregnancy protection than no method at all. The effectiveness of withdrawal depends on the participants' ability to correctly withdraw with every act of sex. As commonly used, about 20 pregnancies per 100 women whose partners use withdrawal over the first year. This means that 80 of every 100 people with uteruses whose partners use withdrawal will not become pregnant. Myth: Health risks and side effects Some people incorrectly believe that using withdrawal will cause health risks and side effects, such as cancer, headaches, or blindness. Fact: Withdrawal does not have any physical side effects for either partner. Myth: Infections Some people mistakenly believe that withdrawal prevents the transmission of sexually transmitted infections (STIs). Fact: Withdrawal does not prevent the transmission of STIs. Lesions or ulcers on the genitals can transmit various infections. Other STIs can be passed from one partner to the other through skin-to-skin contact. If either partner is at risk, the couple should use condoms. The semen of HIV-positive men contains HIV-infected cells and is the primary way that HIV is transmitted through sex. Using withdrawal may reduce the risk of transmitting HIV because the woman is not exposed to semen. Even with withdrawal, however, there is a risk of HIV transmission because the pre-ejaculate fluid may also contain HIV. Studies of heterosexual couples found that the transmission of HIV from male to female was decreased by one-half or more when withdrawal was practiced compared with intercourse with ejaculation inside the woman. No studies have examined whether withdrawal reduces female-to-male transmission of HIV. Myth: Mechanism of action Some people have misconceptions regarding how withdrawal prevents pregnancy, such as incorrectly believing that withdrawal prevents pregnancy by preventing the vagina-owner from having an orgasm. Fact: Practicing withdrawal is not directly related to orgasm. Also, conception does not depend upon whether or not a vagina-owner has an orgasm. Withdrawal prevents pregnancy by preventing sperm from entering the vagina. Myth: Sexual desire and sexual pleasure Some people incorrectly believe that withdrawal will make men infertile, impotent, or weak, or decrease their sex drive. Fact: There is no evidence to suggest that withdrawal will make penis-owners infertile, impotent or weak, or that it will decrease their sex drive. Myth: Who can use the method Some people incorrectly believe that withdrawal is appropriate only for certain people, for instance, only people whose cardiovascular systems function well. Fact: No medical conditions prevent the use of withdrawal. While all men can use this method, its effectiveness depends on the user. Those who ejaculate prematurely or who cannot sense consistently when ejaculation is about to occur may have difficulty using withdrawal. Learning to properly withdraw can take time. Couples may want to use another method until the male feels he can correctly withdraw with every act of sex. Learn more in our video:
11 March 2019
Myths and facts about implants
This page was originally published in 2012 and has since been updated. Contraceptive implants are thin, small (4cm), flexible rods which are implanted under the skin of the upper arm by a doctor or a nurse. They are 99% effective in preventing pregnancy. The implant rods contain progestins which are steadily released into the woman’s bloodstream. Progestins are like the hormone progesterone, which is produced naturally within a woman’s body. The continuous release of progestins stops a woman releasing an egg every month (ovulation), and thickens the mucus from the cervix (neck of the womb), making it difficult for sperm to pass through to the womb and reach an unfertilized egg. Implants protect against pregnancy soon after as they have been inserted. Depending on the type of implant, they last between 3-5 years, but can be removed at any time. Fertility returns when the implant is removed. Some women experience side effects form implants. It is common, but not harmful, to experience changes in menstrual bleeding patterns. Other possible side effects include abdominal pain, headaches, breast tenderness and acne. Side-effects often diminish over time, especially after the first few months to a year of use, but if you are concerned about side effects, you should go and talk to your provider. When fitting the implant, a local anaesthetic is used to numb the area. It makes a small wound in the arm, which is closed with a dressing and does not need stitches. Contraceptive implants do NOT protect against sexually transmitted infections (STIs, including HIV). To protect against STIs, male or female condoms need to be used. Myth: Pregnant while using an implant Some women who seek family planning believe that implants will interrupt an existing pregnancy. Fact: A fetus will not be harmed by the insertion of an implant Implants work primarily by thickening cervical mucus, which blocks sperm from meeting an egg, and by disrupting the menstrual cycle and preventing ovulation. Implants do not interrupt pregnancy. Good evidence shows that implants will not affect the pregnancy or harm the fetus if a woman is already pregnant when implants are inserted or becomes pregnant while using implants. Myth: Getting an implant is painful and could cause infection Some women who seek family planning believe that the insertion of implants requires surgery or that insertion is painful and causes infection. They may also have misconceptions about the removal of implants. Fact: No stitches, no noticeable scar, and it can be removed at any time Health professionals with specific training perform a minor surgical procedure to insert implants. The provider gives the patient an injection of local anesthetic under the skin of her arm to prevent pain while the implants are inserted. This injection may sting. The woman remains fully awake during the procedure. Insertion takes an average of 4 to 5 minutes for Norplant, 2.5 minutes for Jadelle, and 1.5 minutes for Implanon. Insertion can take more or less time, depending on the skill of the provider. The incision is small and stitches are not required. In most cases, insertion does not leave a noticeable scar. Once inserted, the outline of the implants underneath the skin can be felt and sometimes seen. The woman may have bruising and feel pain or soreness for a few days afterward. Infection at the insertion site can occur, but is uncommon. When infection occurs, it is usually within the first two months after insertion. In rare cases, implants may start to come out of the skin. When this occurs, it is usually due to improper insertion or infection. A woman can have her implants removed at any time. Similar to insertion, implant removal is done by a specifically trained provider using local anesthesia and does not require stitches. Removal takes an average of 10 to 15 minutes for Norplant, 5 to 8 minutes for Jadelle, and 3 minutes for Implanon. Removal can take more or less time, depending on the skill of the provider. Difficulties with removal are rare if the implants were properly inserted and the provider is skilled. POLL: Have you tried the implant as a method of contraception?(Please only answer this question if you have the potential to get pregnant. This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)Yes – I currently have one!I used to have one, but not anymoreI've never had an implant Myth: Health risks and side effects Some women who seek family planning do not want to use implants because they have misconceptions about implants causing illness or problems such as cancer, blindness, or birth defects. Fact: Implants have several known health benefits In addition to changes in menstrual bleeding, the most common side effects of implants are headaches, abdominal pain, and breast tenderness. These side effects are not an indication of illness and usually lessen or go away within the first year of use. Studies have not shown increased risk of cancer, blindness or birth defects with the use of implants. They have been shown to greatly reduce the risk of ectopic pregnancy and protect against symptomatic pelvic inflammatory disease. Implants may also help protect against iron-deficiency anemia. Myth: Complications with method Some women who seek family planning believe that implants can cause complications in the arm in which they are inserted or that they can travel from the insertion site to other parts of the body. Fact: Implants cannot travel to other parts of the body They remain where they are inserted until they are removed. In rare cases, a rod may start to come out of the skin, usually during the first four months since insertion. This typically happens because the implants were not inserted well or because of an infection at the insertion site. If expulsion occurs, the woman should return to the clinic as soon as possible and use a back-up family planning method in the meantime. Providers can replace the rods. Myth: Infertility and ectopic pregnancy Some women who seek family planning believe that using implants will cause infertility, delay the return of fertility after the implants are removed, or cause ectopic pregnancies (pregnancy in which the fertilized egg implants in tissue outside the uterus). Fact: Implant doesn't affect your fertility, and reduces the risk of ectopic pregnancy Implants stop working once they are removed and their hormones do not remain in the woman’s body. Implant use does not affect a woman’s ability to become pregnant, although fertility decreases with a woman’s age. One major study found that women who have had their implants removed can become pregnant as quickly as women who have stopped using nonhormonal methods. Implants substantially reduce the risk of ectopic pregnancy. In the United States, the rate of ectopic pregnancy among women who are not using a contraceptive method is 650 ectopic pregnancies per 100,000 women per year. The rate of ectopic pregnancy among women using implants is 6 ectopic pregnancies per 100,000 women per year. Even in the very rare cases when implants fail and pregnancy occurs, the great majority of these pregnancies are not ectopic. Only 10 to 17 of every 100 pregnancies due to the failure of implants are ectopic. Myth: Who can use the method Some women who seek family planning believe that implants should not be used by women who are young or who have not had children. Fact: Nearly all women can use implants safely and effectively Implants are suitable for women of any age, regardless of whether they have had children or not. Implants do not make women infertile—fertility returns as soon as implants are removed. Breastfeeding women can use implants if at least six weeks have passed since they have given birth. Implants may not be suitable for women who require a family planning method without hormones. For example, women who have or have had breast cancer and women with active, serious liver disease should choose an alternative method. Myth: Menstrual bleeding Some women who seek family planning incorrectly believe that using implants will cause harmful changes to menstrual bleeding. Fact: Changes may occur, but generally they are not harmful Changes in menstrual bleeding commonly occur with implant use, but some women do not experience any change. Typically, changes in bleeding patterns are more dramatic during the first year of use and either lessen or stop after the first year. Prolonged or heavy bleeding (lasting over eight days or generating twice as much blood as normal) due to implants generally is not harmful. Menstruation may also cease after one or two years of implant use, which is not harmful either—blood will not build up inside the woman. Myth: Sexual pleasure Some women who seek family planning believe that implants will reduce a woman’s libido or affect a couple’s sexual life in some way. Fact: No evidence to suggest that implants can reduce a woman’s libido There is no evidence to suggest that implants can reduce a woman’s libido. Some women using implants report negative changes in mood and sex drive, while some report improved mood and sex drive. Such changes could be caused by many other factors, so it is difficult to attribute them to implant use. A large majority of implant users do not report any change.
12 June 2012
At a Glance 2010
Key facts and figures highlighting IPPF's achievements in 2009. Sexual and reproductive ill health causes over 30% of the global burden of disease among women of childbearing age and without IPPF, this burden would be even greater.
29 May 2012
IPPF Strategic Framework: 2005 - 2015
The product of a Federation-wide consensus, this framework brings together the ideas and experience of IPPF Member Associations, senior volunteers, Regional Offices and Central Office, and has been approved by the Governing Council. By combining an understanding of our past with a vision for our future, this new plan presents a 'framework of opportunity' that Member Associations can interpret to develop the most appropriate response to specific sexual and reproductive health challenges. The ‘Strategic Framework’ is not intended to impose a rigid set of rules or constraints. Rather, it embraces the diversity of situations Member Associations and regions face. While providing this flexibility, the framework unites the Federation in a common vision on which we are compelled to act if we are to meet the needs of women, men and young people throughout the world.
03 May 2012
IPPF Sexual Rights Declaration Pocket Guide
02 May 2012
Sexual Rights: An IPPF declaration (abridged)
The IPPF declaration is grounded in and informed by international agreements such as United Nations Conventions. This abridged version to be used in conjunction with IPPF's original Sexual Rights Declaration.
11 March 2019
Myths and facts about the Pill
This page was originally published in 2012 and has since been updated. Oral contraceptives (the Pill) are hormonally active pills which are usually taken by women on a daily basis. They contain either two hormones combined (progestogen and estrogen) or a single hormone (progestogen). Combined oral contraceptives suppress ovulation. Progestogen-only contraceptives also suppress ovulation in about half of women (they are slightly less effective). Both types cause a thickening of the cervical mucus, blocking sperm penetration. Oral contraceptives are 92 - 99% effective. A woman can decide to start taking the pill if she is sexually active or planning to become sexually active and is certain she is not pregnant. Some pills are taken daily for 21 days and stopped for 7 days before starting a new package. Other kinds are taken continuously for 28-day cycles. Oral contraceptives should be taken in order, at a convenient and consistent time each day. They are appropriate for women who are willing to use a method that requires action daily and who will be able to obtain supplies on a continuous basis. The pill offers continuous protection against pregnancy, it produces regular and shorter periods (and frequently a decrease in menstrual cramps), and it protects against ovarian and endometrial cancer, ectopic pregnancies and infections of the fallopian tubes. Possible side effects include nausea, breast tenderness, mild headaches, weight gain or loss. Very rarely, it can lead to serious health risks (e.g. blood clots, heart attack, and stroke). Risks are higher for women over 35 years who smoke. The pill does NOT protect against sexually transmitted infections (STIs, including HIV). To protect against STIs, a male or female condom must be used. POLL: Is the Pill your main method of contraception?(Please only answer this question if you have the potential to get pregnant. This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)Yes, I use it at the moment!I used to use it, but not anymoreNo, I've never used it Myth: There is a risk of birth defects Some women who seek family planning incorrectly believe that using COCs will cause birth defects in their babies. Fact: Good evidence shows that COCs will not cause birth defects and will not otherwise harm the fetus if a woman becomes pregnant while taking COCs or accidentally starts to take COCs when she already pregnant. Myth: The contraceptive pill can cause cancer Some women who seek family planning believe that combined oral contraceptives (COCs) cause cancers such as breast cancer, uterine cancer, and ovarian cancer. Fact: The use of combined oral contraceptives (COCs) is proven to decrease the risk of two gynecological cancers (ovarian and endometrial). It is difficult to know the effect of COC use on breast cancer and cervical cancer. The possibly increased risks that have been recorded in some studies are not large enough to outweigh benefits or to change current practice. Use of COCs helps protect women from two kinds of cancers—cancer of the ovaries and cancer of the lining of the uterus (endometrial cancer). This protection continues for 15 or more years after stopping use. Breast cancer Research findings about COCs and breast cancer are difficult to interpret. In studies, breast cancer is slightly more common among women using COCs and those who have used COCs in the past 10 years than among other women. Scientists do not know whether or not COCs actually caused the slight increase in breast cancers. It is possible that the cancers were already there before COC use but were found sooner in COC users. Both COC users and women who do not use COCs can have breast cancer. Cervical cancer Cervical cancer is caused by certain types of human papillomavirus (HPV). HPV is a common STI that usually clears on its own without treatment, but sometimes persists. Use of COCs for five years of more appears to speed up the development of persistent HPV infection into cervical cancer. The number of cervical cancers associated with COC use is thought to be very small. If cervical screening is available, providers can advise COC users—and all other women—to be screened every three years (or as national guidelines recommend) to detect precancerous changes in the cervix, which can be removed. Myth: You will experience general health problems Some women believe that COCs cause hair loss (alopecia), asthma, and headaches. Fact: A woman may experience short term side affects associated with use of combined oral contraceptive (COCs), including changes in bleeding patterns, headaches, and nausea. However such side effects are not a sign of illness, and usually stop within the first few months of using COCs. For a woman whose side effects persist, give her a different COC formulation. In women who are otherwise well, COC use may be continued for many years as there are no adverse effects related to long-term use. In fact, there are also long-term non-contraceptive health benefits of using COCs as they: Help protect against cancer of the lining of the uterus (endometrial cancer) Help protect against cancer of the ovaries Help protect against symptomatic pelvic inflammatory disease May help protect against ovarian cysts May help protect against iron-deficiency anemia Reduce menstrual cramps Reduce menstrual bleeding problems Reduce ovulation pain Reduce excess hair on face or body Reduce symptoms of polycystic ovarian syndrome Reduce symptoms of endometriosis Myth: There is confusion about how often and when to take the pill Some women who seek family planning are misinformed about how often or when they should take the pill. Fact: A woman can start using COCs any time she wants if she is reasonably certain that she is not pregnant. To be reasonably certain a client is not pregnant, providers can use the Pregnancy Checklist. If a client is starting her pack of pills within five days after the start of her menstrual period, there is no need for a backup method as she is immediately protected from pregnancy. If she starts COCs more than five days after the start of her menstrual period, she can start them any time it is reasonably certain she is not pregnant. She will need to use a "back up" method of contraception, such as a male or female condom, for the first seven days of taking pills to ensure protection from pregnancy. The effectiveness of oral contraception depends on a regular intake of the hormones contained in the pill. Therefore pills must be taken daily, until the pack is empty. Although the specific time of day does not matter, the pills should be taken at the same time every day to reduce side effects and to help women remember to take their pills more consistently. The client should be advised not to interrupt taking the pills before a pack is finished, even if she does not have sexual intercourse. If the pills are taken correctly, the client will always start a new pack on the same day of the week. If a client is taking pills from a 21-pill pack, she will wait seven days after taking the last pill in the pack before beginning a new pack. If a client is taking pills from a 28-pill pack, she will take the next pill from the next pack on the very next day. Women do not need to take a “rest” from COCs after taking them for a time. There is no evidence that taking a “rest” is helpful. In fact, taking a”rest” from COCs can lead to unintended pregnancy. COCs can safely be used for many years without having to stop taking them periodically. Myth: There is a risk of infertility, or a delayed return to fertility Women who seek family planning may incorrectly believe that using COCs will cause a long delay in conceiving or prevent them from being able to have children in the future. Fact: The combined oral contraceptive (COC) does not cause infertility. This is true regardless of how long a woman has taken the pill, the number of children the woman has had, or the age of the woman. In fact, some of the non-contraceptive benefits of the pill include preserving fertility by offering protection against pelvic inflammatory disease, endometriosis, and ectopic pregnancy. There is no evidence that COCs delay a woman's return to fertility after she stops taking them. Women who stop using COCs can become pregnant as quickly as women who stop using non-hormonal methods. Myth: Contraceptive pills can get absorbed into the wrong part of the body Many women who seek family planning incorrectly believe that COCs accumulate in the body and cause diseases and tumors, or get stored in the stomach, ovaries, or uterus and form stones. Fact: After the pills are swallowed, they dissolve in the digestive system, and the hormones they contain are absorbed into the bloodstream. After they produce their contraceptive effect, the hormones are metabolised in the liver and gut and are then eliminated from the body. They do not accumulate in the body anywhere. Myth: Contraceptive pills encourage 'promiscuity' Some clients who seek family planning wrongly believe that the pill encourages infidelity, promiscuity, or prostitution in women. Fact: There is no evidence that COCs affect women’s sexual behavior. The evidence on contraception in general shows that sexual behavior is unrelated to contraceptive use. In fact, using contraception shows responsible behavior in order to avoid unintended pregnancy and sexually transmitted infections. Myth: There will be an impact sexual desire and pleasure Some clients who seek family planning may believe that COCs reduce sexual pleasure or interest in sex (loss of libido) or that they cause frigidity in women. Fact: There is no evidence that COCs affect a woman's sex drive. Although some women using the pill have reported either an increase or decrease in sexual interest and performance, it is difficult to say whether such changes are a result of COCs or other life events. Myth: You will experience weight changes Some clients believe that COCs cause women to gain or lose weight. Fact: Most women do not gain or lose weight as a result of COC use. A woman's weight may fluctuate naturally due to changes in age or life circumstance. Because changes in weight are common, many women attribute their natural weight gain or loss to the use of COCs. Although a very small number of COC users may report weight change following COC use, studies have found that, on average, COCs do not affect weight. A few women experience sudden changes in weight when using COCs. These changes reverse after they stop taking COCs. It is not known why these women respond to COCs this way.
11 March 2019
Myths and facts about external condoms
This page was originally published in 2012 and has since been updated. External condoms (sometimes referred to as 'male' condoms) are placed over an erect penis. Learn how to put one on and find out about internal condoms. Back to external condoms – join us as we bust some common myths about this popular contraceptive method. Myth: Complications with method Some clients who seek family planning incorrectly believe that external condoms can easily get lost in a vagina or uterus and can travel through a woman’s body, requiring surgery to get the condom out. Fact: Studies indicate that a condom rarely slips off completely during intercourse. On average, about 2% of condoms break or slip off completely during sex, primarily because they are used incorrectly. Slippage during withdrawal can be minimized if the rim of the condom is held against the base of the penis during withdrawal after ejaculation. However, if a condom does slip, it will go no further than the woman’s vagina, where it can be easily retrieved, with no need for surgery. If a man notices a break or slip, he should tell his partner so that she can use emergency contraceptive pills if she wants. Myth: Effectiveness Some people who seek family planning do not want to use external condoms because they incorrectly believe that condoms are not effective in preventing pregnancy or sexually transmitted infections, including HIV. Fact: The external condom is a sheath, or covering, that fits over an erect penis. It works by forming a barrier that keeps sperm out of the vagina, preventing pregnancy. It also keeps infections that are in semen, on the penis, or in the vagina from infecting the other partner. It is usually made of very thin latex rubber, although a minority are made of either animal tissue or polyurethane (plastic). Condoms are the only contraceptive method that can protect against both pregnancy and sexually transmitted infections (STIs), including HIV transmission, when used for vaginal, oral, or anal sex. In order for condoms to be most effective they must be used correctly and consistently (with every act of sex). The risk of pregnancy or contracting sexually transmitted infections is greatest when condoms are not used correctly with every act of sex. When used correctly and consistently, condoms are 98% effective in preventing pregnancy. This means that when used consistently and correctly, about 2 of every 100 women whose partners use condoms become pregnant over the first year of use. Condoms do not have holes that HIV can pass through. In fact, when used consistently and correctly, condom use prevents 80% to 95% of HIV transmission that would have occurred without condoms. Plastic condoms are expected to provide the same protection as latex condoms, but they have not been studied thoroughly. Condoms made from animal membrane DO NOT protect against HIV and other STIs. On average, about 2% of condoms break or slip off completely during sex, primarily because they are used incorrectly. Used properly, condoms seldom break. Lubrication helps avoid condom breakage. There are three ways to provide lubrication—natural vaginal secretions, adding a lubricant, or using condoms packaged with lubricant on them. Sometimes lubricants made of glycerine or silicone, which are safe to use with latex condoms, are available. Clean water and saliva also can be used for lubrication. Do not use products made with oil as they can damage latex condoms. QUICK POLL: Are external condoms your contraceptive of choice?YesNo Myth: Health risks and side effects Some people incorrectly believe that using external condoms can cause side effects or health risks such as illness, infection, disease, or cancer. Fact: There are no known serious short or long term side effects associated with the use of condoms. When a condom is used, ejaculation occurs as normal, so there is no sperm “back up.” There is no evidence that condoms cause cancer, either in men or women. In fact, the use of condoms may help protect against conditions caused by STIs including recurring pelvic inflammatory disease, cervical cancer, and infertility. It is possible that a person may experience mild irritation in or around the vagina or penis or mild allergic reaction to a condom (itching, redness, rash, and/or swelling of genitals, groin, or thighs during or after condom use). Severe allergic reactions involve hives or rash over much of the body, dizziness, difficulty breathing, or loss of consciousness after coming in contact with latex. Both men and women can be allergic to latex and latex condoms. Allergy to latex is uncommon in the general population, and reports of mild allergic reactions to condoms are very rare. Severe allergic reactions to condoms are extremely rare. Plastic condoms made of synthetic materials offer an alternative for individuals who are allergic or sensitive to latex. Plastic condoms are expected to provide the same protection as latex condoms, but they have not been studied as thoroughly. The United States Food and Drug Administration recommends that condoms made of plastic be used for protection from STIs, including HIV, only if a person cannot use latex condoms. Condoms made of animal skin such as lambskin (also called natural skin condoms) are not effective for preventing STIs, including HIV, however. Myth: Premature ejaculation Some people incorrectly believe that external condoms constrict an erect penis, causing premature ejaculation. Fact: Using an external condom does not cause premature ejaculation. On the contrary, condoms can help users maintain an erection longer and prevent premature ejaculation, especially when the placement of the condom on the penis is a routine part of sexual foreplay. Myth: Promiscuity Some people believe that external condoms encourage infidelity, promiscuity, or prostitution. Fact: There is no evidence that condoms or other methods of contraception affect behavior. The evidence on contraception in general shows that sexual behavior is unrelated to contraceptive use. In fact, using contraception shows responsible behavior in order to avoid unintended pregnancy and sexually transmitted infections. Myth: Sexual Desire and sexual pleasure Some people incorrectly believe that condom use decreases a man’s libido and can cause impotence or that condoms reduce or interfere with sexual pleasure. Fact: There is no evidence to suggest that condom use causes impotence. Impotence has many causes. Some causes are physical, some are emotional. Condoms themselves do not cause impotence. A few men may have problems keeping an erection when using condoms, however. Other men, especially older men, may have difficulty keeping an erection because condoms can dull the sensation of having sex. Using more lubrication may help increase sensation for men using condoms. Some couples become frustrated and lose some of their sexual excitement when they stop to put on a condom. Some men and women complain that the condom dulls sensation. However, many couples learn to enjoy using condoms as part of their sexual foreplay. In fact, many women and men often say they have better sex when they use condoms, because they can focus on their sexual pleasure without the worry about unintended pregnancy and sexually transmitted infections (STIs). A couple may wish to use either a textured, ultra thin, or transparent condom to increase stimulation. Pleasure may also be increased by lubricating the inside and outside of the condom with water-based lubricants. A drop or two of lubricant on the inside of the condom before it is unrolled can help increase the sensation of sex for some men. Too much lubricant inside, however, can make the condom slip off. Lubricants made of glycerine or silicone are safe to use with latex condoms. Clean water and saliva also can be used for lubrication. Do not use products made with oil as lubricants for latex condoms as they can damage latex. External condom use does not interfere with sexual pleasure if the time when you use the condom during intercourse is correct. (Malaysia) If you use condoms correctly they do not interfere with sexual pleasure. (Lithuania) This is not true, please practice using condoms and get experience. (Bangladesh) When using a condom, you forget that you have a condom on your penis. Focus on what you are doing and you will get the same enjoyment. (St. Lucia) External condoms doenot influence the man’s libido or interfere with pleasure. You can use condoms and have the same pleasure. (Central Africa Republic) Myth: Size of penis Some people believe incorrectly that men who have a large penis will not be able to find an external condom that fits them properly. Fact: There are many different kinds and brands of condoms that vary in features such as shape, size, color, lubrication, thickness, texture, and whether or not they are coated with spermicide. Although there are considerable variations between the sizes of individual penises, there is no established market of different sized condoms, even in developed countries. Users should be advised to try different brands to find out which fits best. Condoms of 49mm width are readily available and are the preferred size for a smaller condom. Although there is no “standard” size for larger condoms, some manufacturers produce condoms of 56mm width. Myth: Who can use the method Some people do not want to use external condoms because they incorrectly believe that they should be used only by people in casual relationships, people who have extra marital sexual relations, or by people who have sex for money. Fact: Condoms are an appropriate contraceptive method for anyone, regardless of marital status or sexual behavior, and should be provided to all individuals who request them. While many casual partners rely on condoms for STI protection, married couples all over the world use condoms for pregnancy protection too.
11 March 2019
Myths and facts about the intra-uterine device (IUD)
This page was originally published in 2012 and has since been updated. Myth: Abortion Some couples do not want to use the IUD because they incorrectly believe that the IUD prevents pregnancy by causing abortions. Fact: IUDs do not work by causing abortions In the vast majority of cases, IUDs work by preventing fertilization. The copper-bearing IUD acts as a spermicide, killing or impairing sperm so they cannot reach the egg. IUDs that contain progestin cause the cervical mucus to thicken, which stops sperm from entering the uterus. Thus, the current evidence suggests that the main mechanisms of action of IUDs occur prior to fertilization. In very rare case, IUDs prevent implantation which is considered a contraceptive not an abortifacient effect. Myth: Effectiveness Some women do not want to use the IUD because they incorrectly believe that the IUD is not effective in preventing pregnancy or that the IUD loses its contraceptive effect after only a few years from the time of insertion. Fact: IUDs are the more than 99% effective! Both the hormonal and copper-bearing IUDs are highly effective contraceptive methods. In fact, they are among the most effective reversible methods, with pregnancy rates similar to those for female sterilization. Hormonal levonorgestrel-releasing IUD (LNG-IUD): Less than 1 pregnancy per 100 women using the LNG-IUD over the first year (2 per 1,000 women). That means the LNG-IUD will prevent pregnancy in 998 of 1,000 women. A small risk of pregnancy remains beyond the first year of use and continues as long as the woman is using the LNG-IUD. Over 5 years of LNG-IUD use, about 1 per 100 women (5 to 8 per 1,000 women) will become pregnant. The LNG-IUD is approved for up to 5 years of use. Copper-bearing IUDs: Less than 1 pregnancy per 100 women using an IUD over the first year (6 to 8 per 1,000 women). That means the IUD will prevent pregnancy for 992 to 994 of 1,000 women using IUDs will not become pregnant. A small risk of pregnancy remains beyond the first year of use and continues as long as the woman is using the IUD. Over 10 years of IUD use, about 2 per 100 women will become pregnant. The IUD is effective for up to 12 years. Myth: Health risks and side effects Some women do not want to use the IUD because they incorrectly believe that IUD causes side effects or health risks such as cancer, sexually transmitted infections, or birth defects. Fact: IUDs are safe! Infection related to IUD insertion probably occurs because the instruments or IUD carry with them organisms from the lower genital tract. If the organisms are bacteria normally present in the genital tract, then it seems that some mechanism automatically eliminates this contamination from the uterus soon after the insertion process without infection occurring. Risk of infection can be further reduced by following routine infection-prevention procedures including the “no-touch” insertion technique (not letting the loaded IUD or uterine sounds touch any unsterile surfaces such as hands, speculum, vaginal wall, or table top). The IUD never travels to the heart, brain, or any other part of the body outside the abdomen. The IUD normally stays within the uterus like a seed within a shell. Rarely, the IUD may come through (perforate) the wall of the uterus into the abdominal cavity. This is most often due to a mistake during insertion. Proper insertion technique can help prevent many problems, such as infection, expulsion, and perforation. If uterine perforation is suspected within 6 weeks after insertion or if it is suspected later and is causing symptoms, refer the client for evaluation to a clinician experienced at removing such IUDs. Usually, however, the out-of-place IUD causes no problems and should be left where it is. The woman will need another contraceptive method. POLL: Is an IUD your main method of contraception?(Please only answer this question if you have the potential to get pregnant. This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)Yes, I have one now!I used to have one, but not anymoreNo, I've never had one IUDs do not cause cancer in otherwise healthy women, but confirmed or suspected cancer of the genital tract is a contraindication to IUD use, because the increased risk of infection, perforation, and bleeding at insertion may make the condition worse. For the levonorgestrel-releasing IUD, breast cancer is also a contraindication. IUDs do not increase the risk of contracting STIs, including HIV. However, usually women who have a very high risk of exposure to gonorrhea or chlamydia should not have an IUD inserted. In special circumstances, when other, more appropriate methods are not available or acceptable to her, a qualified provider who can carefully assess a specific woman’s risk may decide that she can use an IUD. IUD use neither causes multiple pregnancies after removal nor increases the risk of birth defects, whether the pregnancy occurs with the IUD in place, or after removal. In the rare event that a client becomes pregnant with an IUD in situ, it is important to explain the risks of leaving the IUD in the uterus during pregnancy. There is a higher risk of preterm delivery or miscarriage, including infected (septic) miscarriage during the first or second trimester, which can be life-threatening. Early removal of the IUD reduces these risks, although the removal procedure itself involves a small risk of miscarriage. There is no evidence of increased risk of fetal malformations, however. Overall levels of Pelvic Inflammatory Disease (PID) in IUD users are low. A woman with chlamydia or gonorrhea at the time of IUD insertion, however, is at higher risk of PID in the first few weeks after insertion than she is later. After the first few weeks, an STI may be no more likely to progress to PID in an IUD user than for other women with STIs. To reduce the risk of infection during IUD insertion, providers can ensure appropriate insertion conditions, screening, and counseling, as well as regularly monitor and treat infection. Antibiotics are usually not routinely given before IUD insertion. Most recent research done where STIs are not common suggests that PID risk is low with or without antibiotics. When appropriate questions to screen for STI risk are asked and IUD insertion is done with proper infection-prevention procedures (including the no-touch insertion technique), there is little risk of infection. Antibiotics may be considered, however, in areas where STIs are common and STI screening is limited. If PID occurs or is suspected with an IUD in place, treatment should be started as soon as possible. There is no need to remove the IUD if a woman wants to continue using it. The PID should be treated and the IUD left in situ. If a woman wants it removed, it can be taken out after starting antibiotic treatment. An IUD should not be inserted in women who currently have a PID. It may be inserted as soon as she finishes treatment, if she is not at risk for reinfection before insertion. The copper in copper-bearing IUDs is not released into the blood. Levels of serum copper in long-term users of copper IUDs are similar to that of the normal population. Myth: Problems after removal Some couples do not want to use the IUD because they incorrectly believe that the IUD will cause infertility, ectopic pregnancy, or miscarriage. Fact: no increased risk of infertility Good studies find no increased risk of infertility among women who have used IUDs, including young women and women with no children. Whether or not a woman has an IUD, however, if she develops pelvic inflammatory disease (PID) and it is not treated, there is some chance that she will become infertile. PID can permanently damage the lining of the fallopian tubes and may partially or totally block one or both tubes enough to cause infertility. Fact: no increased risk of ectopic pregnancy or miscarriage after removal Because any pregnancy among IUD users is rare, ectopic pregnancy among IUD users is even rarer. An IUD does not increase a woman’s overall risk of ectopic pregnancy. In fact, an IUD user’s risk of an ectopic pregnancy is much lower than the risk to a woman who is not using any method of contraception. In the unlikely event of pregnancy in an IUD user, 6 to 8 in every 100 of these pregnancies is ectopic. Thus, the great majority of pregnancies after IUD failure are not ectopic. Still, ectopic pregnancy can be life-threatening, so a provider should be aware that ectopic pregnancy is possible if an IUD fails. IUDs do not cause miscarriages after they have been removed. If correct insertion technique is used, the use of an IUD will not cause any difficulty in future pregnancies. In the rare event that a client becomes pregnant with an IUD in situ, it is important to explain the risks of leaving the IUD in the uterus during pregnancy. There is a higher risk of preterm delivery or first- and second- trimester miscarriage, including infected (septic) miscarriage which can be life-threatening. Early removal of the IUD reduces these risks, although the removal procedure itself involves a small risk of miscarriage. If the client does not want to continue the pregnancy and if therapeutic termination of pregnancy is legally available, inform her accordingly. If she wishes to continue the pregnancy and the IUD strings are visible or can be retrieved safely from the cervical canal, gently remove the IUD or refer for removal. The client should return at once if she develops any signs of miscarriage or septic miscarriage (vaginal bleeding, cramping, pain, abnormal vaginal discharge, or fever). However, if the IUD strings cannot be found in the cervical canal and the IUD cannot be safely retrieved, refer for ultrasound, if possible, to determine whether the IUD is still in the uterus. If the IUD is still in the uterus, if ultrasound is not available, or if the client chooses to keep the IUD, her pregnancy should be followed closely by a nurse or doctor. She should see a nurse or doctor at once if she develops any signs of septic miscarriage. Myth: change of menstrual pattern Many couples do not want to use the IUD because they incorrectly believe that using the IUD will cause either no monthly bleeding (amenorrhea) or heavier, painful, and more frequent menstrual bleeding, and this is harmful for your system. Fact: change in bleeding patterns are not harmful Women can experience changes in bleeding patterns depending on the type of IUD. Women using copper-bearing IUDs may experience: Heavy and prolonged monthly bleeding Irregular bleeding More cramps and pain during monthly bleeding These bleeding changes are normal and usually are not signs of illness. They are most common in the first 3 to 6 months after insertion and usually lessen with time. A provider should evaluate for an underlying condition unrelated to method use if: Cramping continues and occurs between monthly bleeding; Heavy or prolonged bleeding continues, or if bleeding starts suddenly after several months of normal bleeding or long after the IUD was inserted, or; Irregular bleeding persists after 6 months, or starts suddenly after several months of normal bleeding. Severe anaemia requires careful consideration because if heavier menstrual periods are experienced, the additional monthly blood loss could worsen existing anaemia. The anaemia should be treated before an IUD is inserted. The LNG-IUD may actually help to reduce anaemia by reducing blood loss. Women using the LNG-IUD may experience heavy, prolonged, or irregular bleeding in the first few months, but then experience: Lighter, regular, and predictable bleeding Infrequent, light, or no monthly bleeding These bleeding changes also are normal and usually are not signs of illness. Copper-bearing IUDs rarely cause monthly bleeding to stop completely. However, women using an LNG-IUD may not experience monthly bleeding due to strong uniform suppression of the endometrium. If monthly bleeding does not occur while a woman is using a copper-bearing IUD, pregnancy should be excluded. If the woman is not pregnant, other causes of no monthly bleeding should be investigated. Pain associated with menstruation may increase in some women, but usually this is only for the first month or two. The LNG-IUD may reduce the pain associated with menstruation. Non-steroidal anti-inflammatory drugs may also reduce discomfort. Myth: Sexual desire and sexual pleasure Some couples do not want to use the IUD because they incorrectly believe that the IUD will cause inconvenience during sex, pain for the male partner because the strings will hurt the penis, or that using the IUD causes discomfort and pain for the woman during sex. Fact: It might make you more relaxed about unintended pregnancies and enjoy sex even more! There is no reason why an IUD should negatively affect sexual pleasure. On the contrary, being free from fear of pregnancy may allow both partners, especially the woman, to enjoy their sexual life. There is no reason why an IUD should cause discomfort or pain during sexual intercourse unless the woman is already having cramps, which sometimes occur during the first few weeks after insertion. Sexual intercourse cannot displace an IUD. Sometimes a man can feel the strings if they are too long. If this bothers him, cutting the strings shorter should solve the problem. Sometimes a man can also feel discomfort if the strings are cut too short. To remedy the problem, the provider can cut them even shorter so they are not coming out of the cervical canal. The woman should be told beforehand, however, that this will mean she may not be able to feel the strings to check her IUD, and removing her IUD may be more difficult. Alternatively, she can have the IUD replaced with a new one and the strings cut to the correct length. The strings should be cut so that 3 centimeters hang out of the cervix. A man may feel discomfort during sex if the IUD has started to come out through the cervix. If a woman suspects this, she should see a doctor or nurse immediately. Proper counselling of the male partner may be appropriate. Myth: Who can use the method Many women do not want to use the IUD because they incorrectly believe that the IUD should not be used by women who are young or who have not had children. Fact: IUDs are safe for a wide range of women There is no minimum or maximum age requirement for using the IUD. An IUD should be removed after menopause has occurred — at least 12 months after her last monthly bleeding. There is also no requirement that a woman must have children to use the IUD. A history of pelvic infection or multiple sex partners (one indication that a woman is at high risk for STIs) make the choice of an IUD inappropriate for such women. The myth that young women and women without children cannot use IUDs stems from fears about a higher risk of expulsion in these women and fears about a higher risk of infection in these women. Expulsion is more likely in certain circumstances, such as young age at insertion (under 20 or 25 years old). Some studies also have found a higher rate of expulsion among women who have no children. The additional risk of expulsion, however, is not sufficient to deny IUDs to women in these circumstances, because the advantages of the IUD outweigh the risks of expulsion. Women with current gonorrheal or chlamydial infection should not have an IUD inserted. Since laboratory STI tests usually are not available, World Health Organization guidance considers STI risk assessment and physical examination essential to safe use of IUDs, but not laboratory tests. Providers should not determine a woman’s STI risk based on her age or whether she has had children. Rather, the provider can discuss risky behaviors or situations in their communities that they think are most likely to expose women to STIs, for example having more than one sexual partner in the last three months without always using condoms. The client can think about whether such situations occurred recently (in the past 3 months or so).
11 March 2019
Myths and facts about female sterilization
This page was originally published in 2012 and has since been updated. Female sterilization is an effective form of contraception that permanently prevents a woman from becoming pregnant. Sterilization does NOT protect against sexually transmitted infections (STIs), including HIV. The operation involves cutting or blocking the fallopian tubes, which carry eggs from the ovaries to the womb. This prevents the eggs from reaching the sperm and becoming fertilized. It can be a fairly minor operation, with many women returning home the same day. In most cases, female sterilization is more than 99% effective, and all women can be sterilized. However, sterilization should only be considered by women who do not want any more children, or who do not want children at all. Once a woman is sterilized, it is very difficult to reverse the process. Couples often decide upon sterilization mutually, when they both feel they do not want any more children. If a couple decides upon sterilization as their preferred contraceptive method, either partner could be sterilized. If both options are acceptable, vasectomy is preferable. It is simpler, safer, easier and less expensive. Myth: Sterilization causes cancer Some clients incorrectly believe that female sterilization will cause women to develop cancer of the reproductive organs (uterus, cervix, or ovaries). Fact: Female sterilization does not increase the risk of cancer of the reproductive organs which are defined below. Very little research has been done to investigate the relationship between breast cancer and female sterilization, but so far there is no evidence of such a link. Myth: All of a woman's reproductive organs will be removed Some clients incorrectly believe that female sterilization involves the removal of some or all of a woman’s reproductive organs, including the vagina. Fact: During the sterilization procedure, the ovaries, uterus, and cervix are left in place. Only the fallopian tubes (the tubes which carry eggs from the ovaries to the uterus) are blocked or cut. The two most common surgical approaches are laparoscopy and minilaparotomy. POLL: Have you undergone female sterlisation as a method of contraception?(Please only answer this question if you have the potential to get pregnant. This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)YesNo Myth: There are health risks and side effects Some clients incorrectly believe that female sterilization leads to health risks or side effects such as hysterectomy, poor health, pain, changes in menstrual bleeding or hormonal imbalances. Fact: There are no documented medical side effects of female sterilization. The few complications that do occur during or following sterilization, such as infection or abscess of the wound, can generally be kept to a minimum if appropriate techniques are used and if the procedure if performed in an appropriate setting. Local anesthesia is best for female sterilization because it has lower risks of complications than use of general anesthesia. The risks are lowest when local anesthesia is used without sedatives. If sedatives are used, providers should closely monitor the woman’s vital signs, such as pulse rate and blood pressure throughout the procedure. Also, most research finds no major changes in menstrual bleeding patterns after female sterilization. Myth: Sterilization means a woman will no longer ovulate Some people incorrectly believe that female sterilization prevents pregnancy either by stopping ovulation or by killing a woman’s egg. Fact: Female sterilization does not stop ovulation or harm a woman’s egg in any way. An egg will still be released each month, but it will dissolve and be reabsorbed by the body. Myth: You will lose your sex drive Some clients incorrectly believe that female sterilization causes women to lose their sex drive or lose their sexual ability. Fact: After sterilization a woman will look and feel the same as before. There is no loss of sexual drive or interest after female sterilization. She can have sex the same as before. She may find that sex is more enjoyable because she does not have to worry about getting pregnant. Myth: You will experience weight changes Some clients incorrectly believe that female sterilization will cause women to lose weight or to gain weight or that female sterilization will disfigure a woman’s body. Fact: Sterilization does not cause any changes in weight, appetite, or appearance. However, older women are more likely to choose sterilization for contraception than younger women and most women gain weight as they age. Myth: Only certain women can undergo sterilization Some women avoid female sterilization because they incorrectly believe that only women of a certain age or who have a certain number of children can undergo female sterilization. Fact: All women can have female sterilization. No medical conditions prevent a woman from using female sterilization.
30 January 2018
Myths and facts about the withdrawal method
This page was originally published in 2012 and has since been updated. Withdrawal (also known as 'pulling out') is when the a penis is removed from a vagina before ejaculation. This prevents the semen from entering the vagina-owner's body. However, even if the penis is withdrawn before ejaculation, pre-ejaculate fluid may contain sperm cells that can cause pregnancy and it may also contain organisms that cause sexually transmitted infections (STIs), including HIV. Withdrawal is not recommended as a main method of contraception. It is dependent on the penis-owner, it requires great self-control, self-awareness and motivation, it may affect sexual pleasure, and it provides no protection against STIs. People are advised to use withdrawal only if both partners are prepared to deal with the consequences of a pregnancy. Blog: Learn more about pre-ejaculatory fluid and if it can cause pregnancy Myth: Correct method use Some people have misconceptions about how to use withdrawal correctly. For example, people incorrectly believe that the clear fluid that comes out of a penis before ejaculation (pre-ejaculate fluid) can cause pregnancy. Fact: As the pre-ejaculate leaves the body, however, it may pick up sperm from a previous ejaculation that remains in the urethra. One study found small clumps of sperm in the pre-ejaculate fluid of some participants. Though only a few hundred sperm were present, they could theoretically pose a low risk of pregnancy. POLL: Have you ever tried withdrawal as a method of contraception?(This poll is completely confidential, and responses do not reflect IPPF's recommendations of this particular method.)Yes – I do it all the timeYes, I've tried it but don't use it regularlyNo, never! Such small amounts of sperm can likely be flushed out with urination, although no research has verified this. If a person using withdrawal has ejaculated recently, they should urinate and wipe the tip of their penis to remove any remaining sperm before having sex again. Myth: Effectiveness Some people have misconceptions about the effectiveness of withdrawal. Fact: Withdrawal is one of the least effective contraceptive methods - although it offers better pregnancy protection than no method at all. The effectiveness of withdrawal depends on the participants' ability to correctly withdraw with every act of sex. As commonly used, about 20 pregnancies per 100 women whose partners use withdrawal over the first year. This means that 80 of every 100 people with uteruses whose partners use withdrawal will not become pregnant. Myth: Health risks and side effects Some people incorrectly believe that using withdrawal will cause health risks and side effects, such as cancer, headaches, or blindness. Fact: Withdrawal does not have any physical side effects for either partner. Myth: Infections Some people mistakenly believe that withdrawal prevents the transmission of sexually transmitted infections (STIs). Fact: Withdrawal does not prevent the transmission of STIs. Lesions or ulcers on the genitals can transmit various infections. Other STIs can be passed from one partner to the other through skin-to-skin contact. If either partner is at risk, the couple should use condoms. The semen of HIV-positive men contains HIV-infected cells and is the primary way that HIV is transmitted through sex. Using withdrawal may reduce the risk of transmitting HIV because the woman is not exposed to semen. Even with withdrawal, however, there is a risk of HIV transmission because the pre-ejaculate fluid may also contain HIV. Studies of heterosexual couples found that the transmission of HIV from male to female was decreased by one-half or more when withdrawal was practiced compared with intercourse with ejaculation inside the woman. No studies have examined whether withdrawal reduces female-to-male transmission of HIV. Myth: Mechanism of action Some people have misconceptions regarding how withdrawal prevents pregnancy, such as incorrectly believing that withdrawal prevents pregnancy by preventing the vagina-owner from having an orgasm. Fact: Practicing withdrawal is not directly related to orgasm. Also, conception does not depend upon whether or not a vagina-owner has an orgasm. Withdrawal prevents pregnancy by preventing sperm from entering the vagina. Myth: Sexual desire and sexual pleasure Some people incorrectly believe that withdrawal will make men infertile, impotent, or weak, or decrease their sex drive. Fact: There is no evidence to suggest that withdrawal will make penis-owners infertile, impotent or weak, or that it will decrease their sex drive. Myth: Who can use the method Some people incorrectly believe that withdrawal is appropriate only for certain people, for instance, only people whose cardiovascular systems function well. Fact: No medical conditions prevent the use of withdrawal. While all men can use this method, its effectiveness depends on the user. Those who ejaculate prematurely or who cannot sense consistently when ejaculation is about to occur may have difficulty using withdrawal. Learning to properly withdraw can take time. Couples may want to use another method until the male feels he can correctly withdraw with every act of sex. Learn more in our video: